Department of Psychology, BioImaging Research Center, University of Georgia, Athens, GA 30602, United States of America.
Department of Medicine, Section of Hospital Medicine, University of Chicago, Chicago, IL, United States of America.
Schizophr Res. 2023 Oct;260:143-151. doi: 10.1016/j.schres.2023.08.006. Epub 2023 Aug 30.
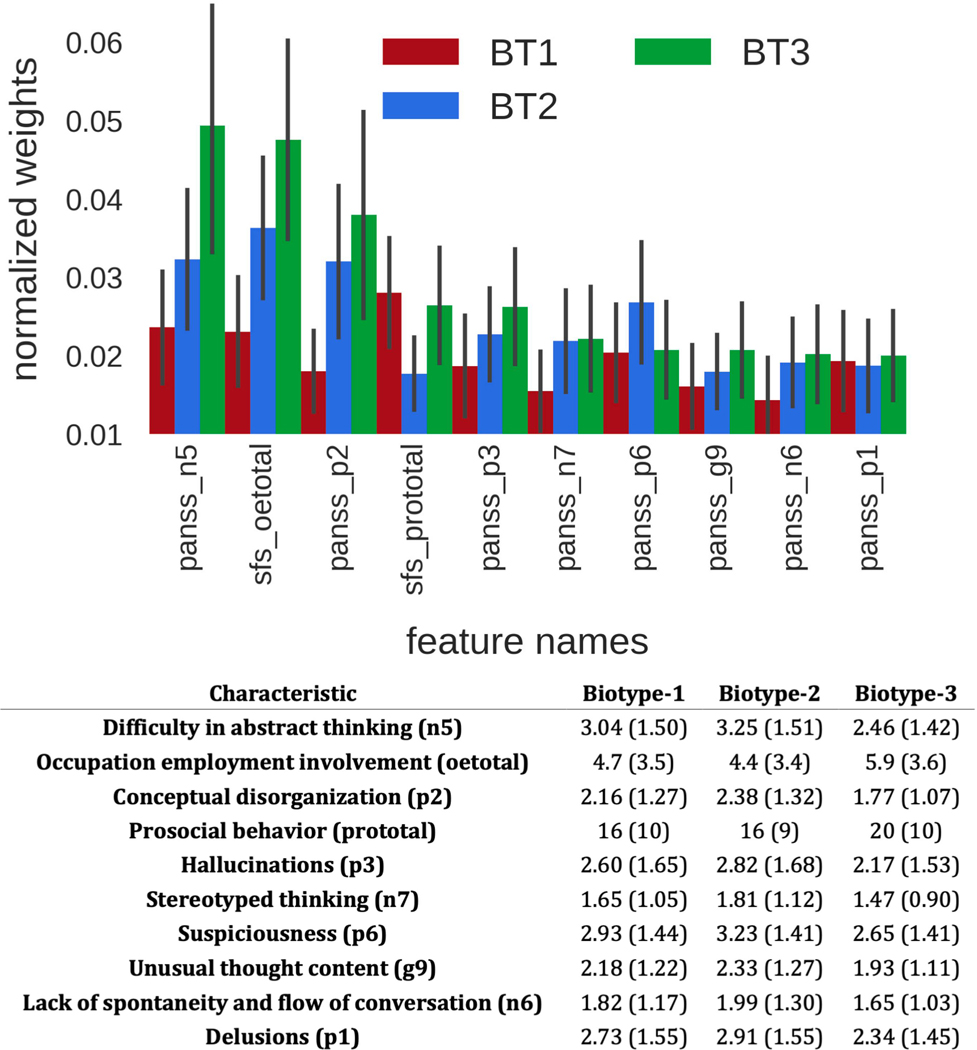
Clinically defined psychosis diagnoses are neurobiologically heterogeneous. The B-SNIP consortium identified and validated more neurobiologically homogeneous psychosis Biotypes using an extensive battery of neurocognitive and psychophysiological laboratory measures. However, typically the first step in any diagnostic evaluation is the clinical interview. In this project, we evaluated if psychosis Biotypes have clinical characteristics that can support their differentiation in addition to obtaining laboratory testing. Clinical interview data from 1907 individuals with a psychosis Biotype were used to create a diagnostic algorithm. The features were 58 ratings from standard clinical scales. Extremely randomized tree algorithms were used to evaluate sensitivity, specificity, and overall classification success. Biotype classification accuracy peaked at 91 % with the use of 57 items on average. A reduced feature set of 28 items, though, also showed 81 % classification accuracy. Using this reduced item set, we found that only 10-11 items achieved a one-vs-all (Biotype-1 or not, Biotype-2 or not, Biotype-3 or not) area under the sensitivity-specificity curve of .78 to .81. The top clinical characteristics for differentiating psychosis Biotypes, in order of importance, were (i) difficulty in abstract thinking, (ii) multiple indicators of social functioning, (iii) conceptual disorganization, (iv) severity of hallucinations, (v) stereotyped thinking, (vi) suspiciousness, (vii) unusual thought content, (viii) lack of spontaneous speech, and (ix) severity of delusions. These features were remarkably different from those that differentiated DSM psychosis diagnoses. This low-burden adaptive algorithm achieved reasonable classification accuracy and will support Biotype-specific etiological and treatment investigations even in under-resourced clinical and research environments.
临床上定义的精神病诊断具有神经生物学异质性。B-SNIP 联盟使用广泛的神经认知和心理生理学实验室测量方法,确定并验证了更多神经生物学同质的精神病生物型。然而,通常在任何诊断评估的第一步都是临床访谈。在这个项目中,我们评估了精神病生物型是否具有临床特征,可以支持除获得实验室测试外对其进行区分。使用来自 1907 名精神病生物型个体的临床访谈数据创建了一个诊断算法。特征是来自标准临床量表的 58 个评分。使用极端随机树算法评估了敏感性、特异性和总体分类成功率。生物型分类准确率最高达到 91%,平均使用 57 个项目。尽管使用了 28 个项目的简化特征集,但分类准确率仍达到 81%。使用这个简化项目集,我们发现只有 10-11 个项目达到了一种一对比所有(生物型 1 或不是,生物型 2 或不是,生物型 3 或不是)的敏感性特异性曲线下面积为.78 到.81。区分精神病生物型的最重要的临床特征依次为:(i)抽象思维困难,(ii)多种社会功能指标,(iii)概念混乱,(iv)幻觉严重程度,(v)刻板思维,(vi)多疑,(vii)异常思维内容,(viii)自发性言语缺乏,和(ix)妄想严重程度。这些特征与区分 DSM 精神病诊断的特征明显不同。这种低负担的自适应算法实现了合理的分类准确性,即使在资源匮乏的临床和研究环境中,也将支持针对生物型的病因和治疗研究。