National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, UK.
Centre for Health Policy, Melbourne School of Population and Global Health, The University of Melbourne, Parkville, VIC, Australia.
Hum Reprod. 2023 Dec 4;38(12):2507-2515. doi: 10.1093/humrep/dead198.
Is the long-term health care utilization of children born after ART more costly to the healthcare system in England than children born to mothers with no fertility problems?
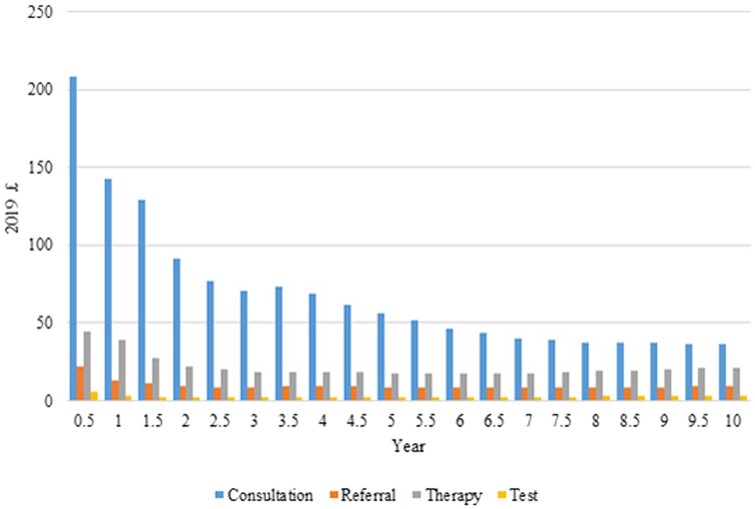
Children born after ART had significantly more general practitioner (GP) consultations and higher primary care costs up to 10 years after birth, and significantly higher hospital admission costs in the first year after birth, compared to children born to mothers with no fertility problems.
There is evidence that children born after ART are at an increased risk of adverse birth outcomes and a small increased risk of rare adverse outcomes in childhood.
STUDY DESIGN, SIZE, DURATION: We conducted a longitudinal study of 368 088 mother and baby pairs in England using a bespoke linked dataset. Singleton babies born 1997-2018, and their mothers, who were registered at GP practices in England contributing data to the Clinical Practice Research Datalink (CPRD), were identified through the CPRD GOLD mother-baby dataset; this data was augmented with further linkage to the mothers' Human Fertilisation and Embryology Authority (HFEA) Register data. Four groups of babies were identified through the mothers' records: a 'fertile' comparison group, an 'untreated sub-fertile' group, an 'ovulation induction' group, and an ART group. Babies were followed-up from birth to 28 February 2021, unless censored due to loss to follow-up (e.g. leaving GP practice, emigration) or death.
PARTICIPANTS/MATERIALS, SETTING, METHODS: The CPRD collects anonymized coded patient electronic health records from a network of GPs in the UK. We estimated primary care costs and hospital admission costs for babies in the four fertility groups using the CPRD GOLD data and the linked Hospital Episode Statistics (HES) Admitted Patient Care (APC) data. Linear regression was used to compare the care costs in the different groups. Inverse probability weights were generated and applied to adjust for potential bias caused by attrition due to loss to follow-up.
Children born to mothers with no fertility problems had significantly fewer consultations and lower primary care costs compared to the other groups throughout the 10-years' follow up. Regarding hospital costs, children born after ART had significantly higher hospital admission costs in the first year after birth compared to those born to mothers with no fertility problems (difference = £307 (95% CI: 153, 477)). The same pattern was observed in children born after untreated subfertility and ovulation induction.
LIMITATIONS, REASONS FOR CAUTION: HFEA linkage uses non-donor data cycles only, and the introduction of consent for data use reduced the availability of HFEA records after 2009. The fertility groups were derived by augmenting HFEA data with evidence from primary care records; however, there remains some potential misclassification of exposure groups. The cost of neonatal critical care is not captured in the HES APC data, which may cause underestimation of the cost differences between the comparison group and the infertility groups.
The findings can help anticipate the financial impact on the healthcare system associated with subfertility and ART, particularly as the demand for these treatments grows.
STUDY FUNDING/COMPETING INTEREST(S): C.C. and this work were funded by a UK Medical Research Council Career Development Award [MR/L019671/1] and a UK MRC Transition Support Award [MR/W029286/1]. X.H. is an Australia National Health and Medical Research Council (NHMRC) Emerging Leadership Fellow [grant number 2009253]. The authors declare no competing interest.
N/A.
英国接受辅助生殖技术(ART)出生的儿童与没有生育问题的母亲所生的儿童相比,其长期医疗保健利用是否对医疗保健系统的成本更高?
与没有生育问题的母亲所生的儿童相比,接受 ART 出生的儿童在出生后 10 年内接受全科医生(GP)咨询的次数更多,初级保健费用更高,并且在出生后的第一年住院费用更高。
有证据表明,接受 ART 出生的儿童出生结局不良的风险增加,并且在儿童期罕见不良结局的风险略有增加。
研究设计、规模、持续时间:我们使用定制的关联数据集,对英格兰的 368088 对母婴进行了纵向研究。通过 CPRD GOLD 母婴数据集,从英格兰参与临床实践研究数据链接(CPRD)的 GP 实践中确定了 1997 年至 2018 年出生的单胎婴儿及其母亲;通过进一步与母亲的人类受精和胚胎管理局(HFEA)登记处的数据进行链接,增加了这一数据。通过母亲的记录确定了四个婴儿组:一个“健康”对照组、一个“未经治疗的轻度不育”组、一个“排卵诱导”组和一个 ART 组。从出生到 2021 年 2 月 28 日对婴儿进行随访,除非因随访丢失(例如离开 GP 实践、移民)或死亡而被剔除。
参与者/材料、设置、方法:CPRD 从英国的 GP 网络中收集匿名编码的患者电子健康记录。我们使用 CPRD GOLD 数据和关联的医院入院统计数据(HES)入院患者护理(APC)数据,估计了四个生育组中婴儿的初级保健费用和住院费用。使用线性回归比较了不同组的护理费用。生成了逆概率权重,并应用于调整因随访丢失导致的潜在偏倚。
与其他组相比,没有生育问题的母亲所生的儿童在整个 10 年的随访中接受的咨询次数较少,初级保健费用也较低。关于住院费用,与没有生育问题的母亲所生的儿童相比,接受 ART 出生的儿童在出生后的第一年住院费用显著更高(差异=£307(95%CI:153,477))。未治疗的轻度不育和排卵诱导组也观察到了同样的模式。
局限性、谨慎的原因:HFEA 链接仅使用非供体数据周期,并且在 2009 年之后,数据使用同意书的引入降低了 HFEA 记录的可用性。通过与初级保健记录中的证据相结合,对 HFEA 数据进行了扩充,从而确定了暴露组;但是,暴露组的分类仍然存在一些潜在的错误。HES APC 数据未捕获新生儿重症监护的费用,这可能导致对对照组和不育组之间成本差异的低估。
这些发现可以帮助预测与生育力低下和 ART 相关的医疗保健系统的财务影响,特别是随着这些治疗方法的需求增长。
研究资助/利益冲突:C.C. 和这项工作得到了英国医学研究理事会职业发展奖(MR/L019671/1)和英国医学研究理事会过渡支持奖(MR/W029286/1)的资助。X.H. 是澳大利亚国家健康与医学研究理事会(NHMRC)新兴领导力研究员(grant number 2009253)。作者没有竞争利益。
无。