Center for Evidence-Based and Translational Medicine, Zhongnan Hospital of Wuhan University, Wuhan, China.
Department of Urology, The First People's Hospital of Tianmen in Hubei Province, The Affiliated Hospital of Hubei University of Science and Technology, Tianmen, China.
BMC Public Health. 2024 Mar 25;24(1):891. doi: 10.1186/s12889-024-18353-9.
Bladder, kidney and prostate cancers make significant contributors to cancer burdens. Exploring their cross-country inequalities may inform equitable strategies to meet the 17 sustainable development goals before 2030.
We analyzed age-standardized disability-adjusted life-years (ASDALY) rates for the three cancers based on Global Burden of Diseases Study 2019. We quantified the inequalities using slope index of inequality (SII, absolute measure) and concentration index (relative measure) associated with national sociodemographic index.
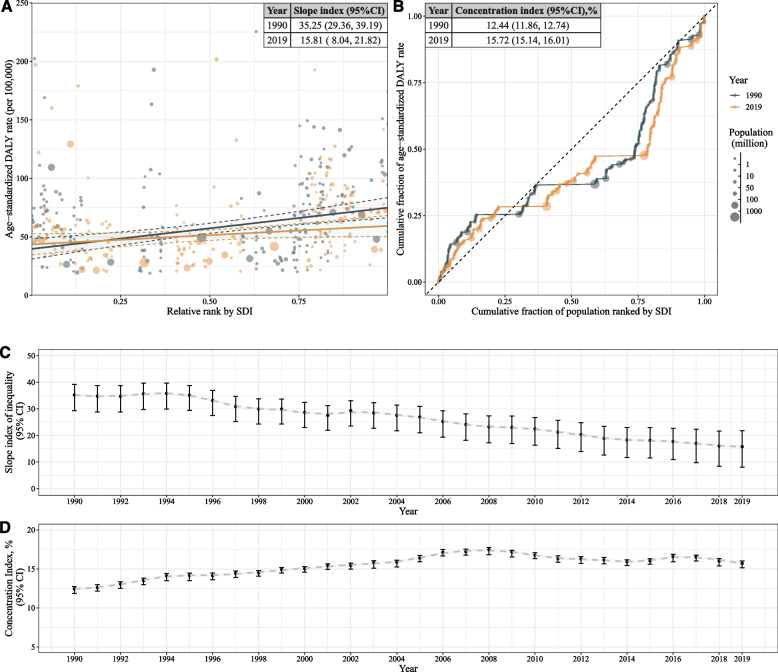
Varied ASDALY rates were observed in the three cancers across 204 regions. The SII decreased from 35.15 (95% confidence interval, CI: 29.34 to 39.17) in 1990 to 15.81 (95% CI: 7.99 to 21.79) in 2019 for bladder cancers, from 78.94 (95% CI: 75.97 to 81.31) in 1990 to 59.79 (95% CI: 55.32 to 63.83) in 2019 for kidney cancer, and from 192.27 (95% CI: 137.00 to 241.05) in 1990 to - 103.99 (95% CI: - 183.82 to 51.75) in 2019 for prostate cancer. Moreover, the concentration index changed from 12.44 (95% CI, 11.86 to 12.74) in 1990 to 15.72 (95% CI, 15.14 to 16.01) in 2019 for bladder cancer, from 33.88 (95% CI: 33.35 to 34.17) in 1990 to 31.13 (95% CI: 30.36 to 31.43) in 2019 for kidney cancer, and from 14.61 (95% CI: 13.89 to 14.84) in 1990 to 5.89 (95% CI: 5.16 to 6.26) in 2019 for prostate cancer. Notably, the males presented higher inequality than females in both bladder and kidney cancer from 1990 to 2019.
Different patterns of inequality were observed in the three cancers, necessitating tailored national cancer control strategies to mitigate disparities. Priority interventions for bladder and kidney cancer should target higher socioeconomic regions, whereas interventions for prostate cancer should prioritize the lowest socioeconomic regions. Additionally, addressing higher inequality in males requires more intensive interventions among males from higher socioeconomic regions.
膀胱癌、肾癌和前列腺癌是癌症负担的主要来源。研究它们在国家间的不平等现象,可以为 2030 年之前实现 17 项可持续发展目标提供公平的策略。
我们根据 2019 年全球疾病负担研究分析了这三种癌症的年龄标准化残疾调整生命年(ASDALY)率。我们使用斜率指数不平等(SII,绝对衡量)和与国家社会人口指数相关的集中指数(相对衡量)来衡量不平等。
在 204 个地区观察到三种癌症的 ASDALY 率存在差异。1990 年至 2019 年,膀胱癌的 SII 从 35.15(95%置信区间:29.34-39.17)降至 15.81(95%置信区间:7.99-21.79),肾癌从 78.94(95%置信区间:75.97-81.31)降至 59.79(95%置信区间:55.32-63.83),前列腺癌从 192.27(95%置信区间:137.00-241.05)降至-103.99(95%置信区间:-183.82-51.75)。此外,1990 年至 2019 年,膀胱癌的集中指数从 12.44(95%置信区间,11.86-12.74)变为 15.72(95%置信区间,15.14-16.01),肾癌从 33.88(95%置信区间:33.35-34.17)变为 31.13(95%置信区间:30.36-31.43),前列腺癌从 14.61(95%置信区间:13.89-14.84)变为 5.89(95%置信区间:5.16-6.26)。值得注意的是,1990 年至 2019 年,男性在膀胱癌和肾癌中的不平等程度均高于女性。
三种癌症的不平等模式存在差异,需要制定有针对性的国家癌症控制策略来减轻差异。膀胱癌和肾癌的优先干预措施应针对社会经济水平较高的地区,而前列腺癌的干预措施应优先考虑社会经济水平较低的地区。此外,解决男性更高的不平等问题需要在来自较高社会经济地区的男性中进行更深入的干预。