Centre de recherche du Centre hospitalier de l'Université de Montréal (CRCHUM), Montréal, QC, Canada.
Department of Radiology, CISSS des Laurentides, Hôpital de Saint-Eustache, Saint-Eustache, QC, Canada.
PLoS One. 2024 Sep 11;19(9):e0307815. doi: 10.1371/journal.pone.0307815. eCollection 2024.
The purpose of this study was to determine and compare the performance of pre-treatment clinical risk score (CRS), radiomics models based on computed (CT), and their combination for predicting time to recurrence (TTR) and disease-specific survival (DSS) in patients with colorectal cancer liver metastases.
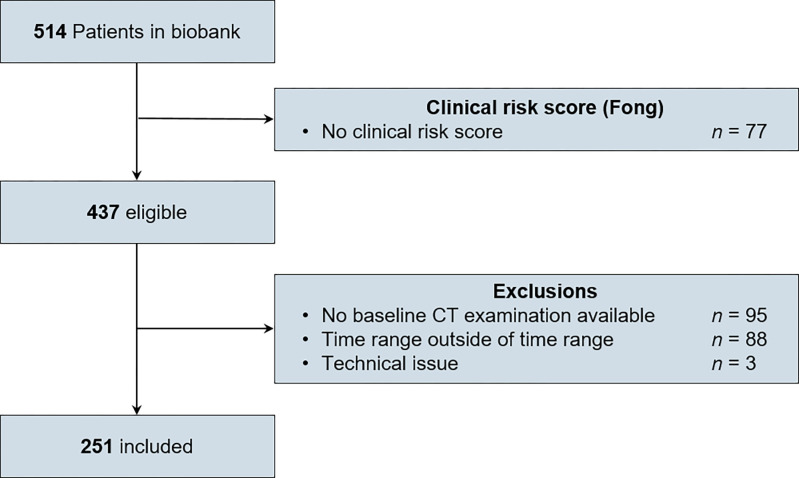
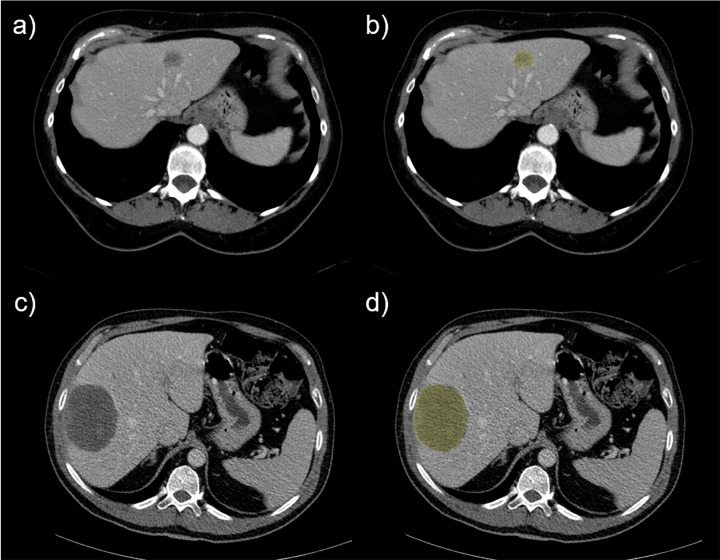
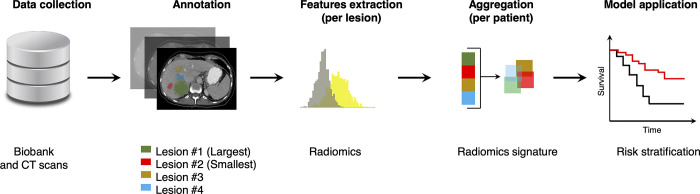
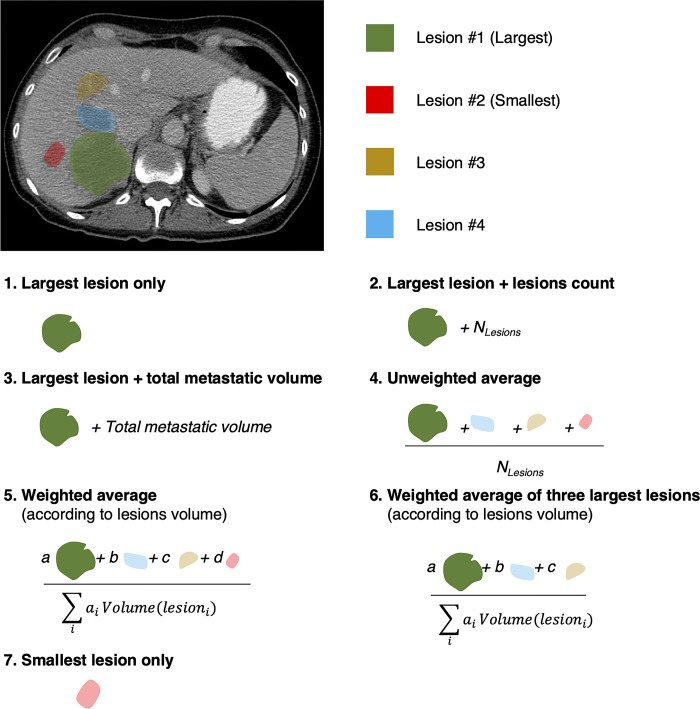
We retrospectively analyzed a prospectively maintained registry of 241 patients treated with systemic chemotherapy and surgery for colorectal cancer liver metastases. Radiomics features were extracted from baseline, pre-treatment, contrast-enhanced CT images. Multiple aggregation strategies were investigated for cases with multiple metastases. Radiomics signatures were derived using feature selection methods. Random survival forests (RSF) and neural network survival models (DeepSurv) based on radiomics features, alone or combined with CRS, were developed to predict TTR and DSS. Leveraging survival models predictions, classification models were trained to predict TTR within 18 months and DSS within 3 years. Classification performance was assessed with area under the receiver operating characteristic curve (AUC) on the test set.
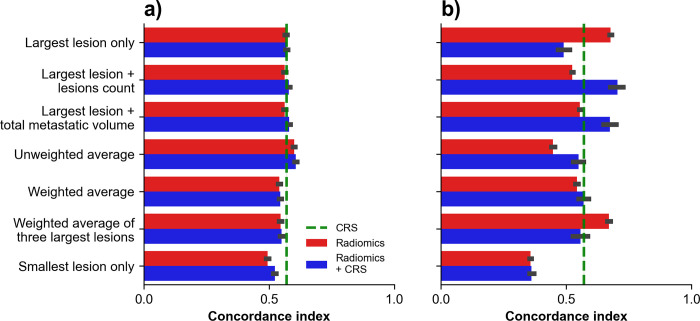
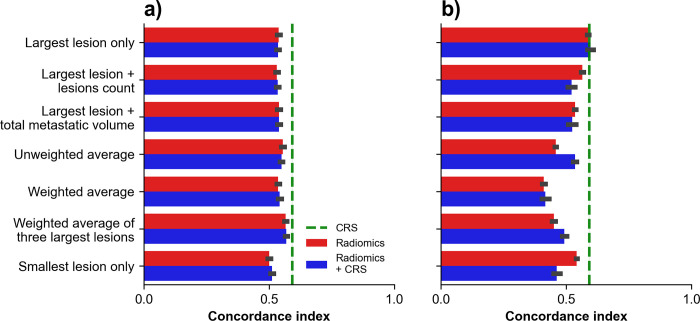
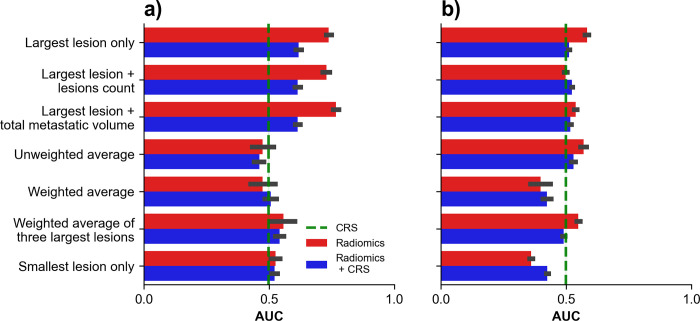
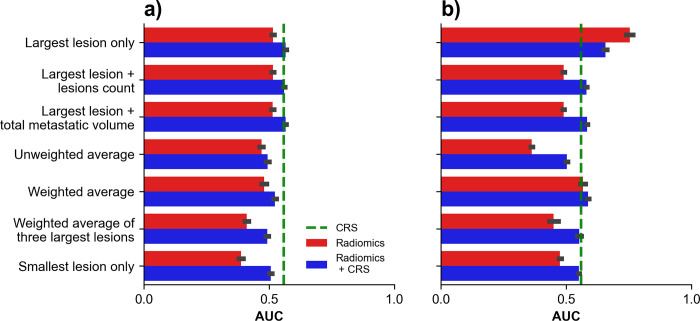
For TTR prediction, the concordance index (95% confidence interval) was 0.57 (0.57-0.57) for CRS, 0.61 (0.60-0.61) for RSF in combination with CRS, and 0.70 (0.68-0.73) for DeepSurv in combination with CRS. For DSS prediction, the concordance index was 0.59 (0.59-0.59) for CRS, 0.57 (0.56-0.57) for RSF in combination with CRS, and 0.60 (0.58-0.61) for DeepSurv in combination with CRS. For TTR classification, the AUC was 0.33 (0.33-0.33) for CRS, 0.77 (0.75-0.78) for radiomics signature alone, and 0.58 (0.57-0.59) for DeepSurv score alone. For DSS classification, the AUC was 0.61 (0.61-0.61) for CRS, 0.57 (0.56-0.57) for radiomics signature, and 0.75 (0.74-0.76) for DeepSurv score alone.
Radiomics-based survival models outperformed CRS for TTR prediction. More accurate, noninvasive, and early prediction of patient outcome may help reduce exposure to ineffective yet toxic chemotherapy or high-risk major hepatectomies.
本研究旨在确定和比较治疗前临床风险评分(CRS)、基于计算机断层扫描(CT)的放射组学模型及其组合在预测结直肠癌肝转移患者复发时间(TTR)和疾病特异性生存(DSS)方面的性能。
我们回顾性分析了 241 例接受结直肠癌肝转移系统化疗和手术治疗的患者前瞻性维护的登记处。从基线、治疗前、对比增强 CT 图像中提取放射组学特征。对于多个转移灶的病例,研究了多种聚合策略。使用特征选择方法得出放射组学特征。使用随机生存森林(RSF)和基于放射组学特征的神经网络生存模型(DeepSurv),单独或与 CRS 联合,预测 TTR 和 DSS。利用生存模型预测,在测试集中利用分类模型对 18 个月内 TTR 和 3 年内 DSS 进行预测。使用接收器操作特征曲线(ROC)下面积(AUC)评估分类性能。
对于 TTR 预测,CRS 的一致性指数(95%置信区间)为 0.57(0.57-0.57),CRS 联合 RSF 为 0.61(0.60-0.61),CRS 联合 DeepSurv 为 0.70(0.68-0.73)。对于 DSS 预测,CRS 的一致性指数为 0.59(0.59-0.59),CRS 联合 RSF 为 0.57(0.56-0.57),CRS 联合 DeepSurv 为 0.60(0.58-0.61)。对于 TTR 分类,CRS 的 AUC 为 0.33(0.33-0.33),放射组学特征的 AUC 为 0.77(0.75-0.78),DeepSurv 评分的 AUC 为 0.58(0.57-0.59)。对于 DSS 分类,CRS 的 AUC 为 0.61(0.61-0.61),放射组学特征的 AUC 为 0.57(0.56-0.57),DeepSurv 评分的 AUC 为 0.75(0.74-0.76)。
基于放射组学的生存模型在 TTR 预测方面优于 CRS。对患者预后进行更准确、无创和早期预测,可能有助于减少无效但有毒的化疗或高风险的大肝切除术的暴露。