Cho Sung-Min, Khanduja Shivalika, Wilcox Christopher, Dinh Kha, Kim Jiah, Kang Jin Kook, Chinedozi Ifeanyi David, Darby Zachary, Acton Matthew, Rando Hannah, Briscoe Jessica, Bush Errol L, Sair Haris I, Pitts John, Arlinghaus Lori R, Wandji Audrey-Carelle N, Moreno Elena, Torres Glenda, Akkanti Bindu, Gavito-Higuera Jose, Keller Steven, Choi HuiMahn A, Kim Bo Soo, Gusdon Aaron, Whitman Glenn J
Department of Surgery, Division of Cardiac Surgery (S.-M.C., S.K., C.W., J.K.K., I.D.C., Z.D., M.A., H.R., J.B., S.K., B.S.K., G.J.W.), Johns Hopkins University School of Medicine, Baltimore, MD.
Departments of Neurology, Neurosurgery, and Anesthesiology and Critical Care Medicine, Neuroscience Critical Care Division (S.-M.C., J.K.), Johns Hopkins University School of Medicine, Baltimore, MD.
Circulation. 2024 Dec 10;150(24):1955-1965. doi: 10.1161/CIRCULATIONAHA.124.069187. Epub 2024 Sep 29.
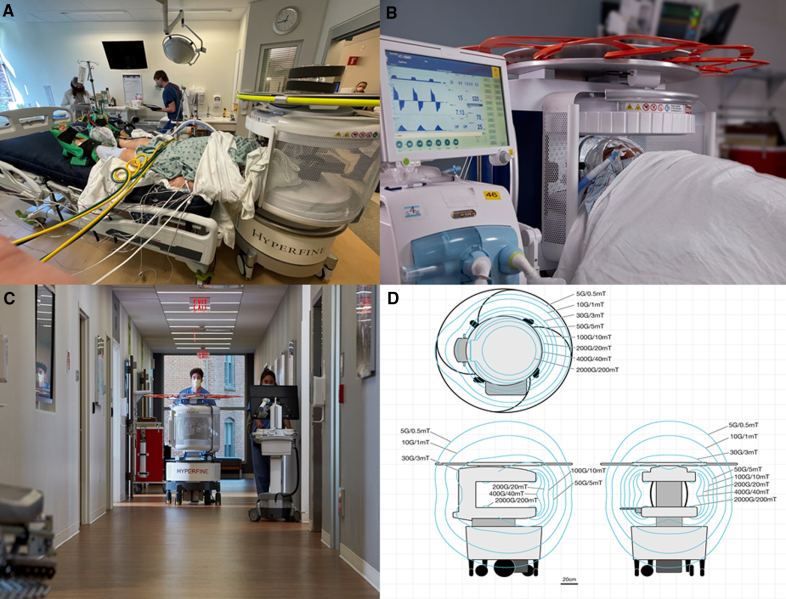
Early detection of acute brain injury (ABI) at the bedside is critical in improving survival for patients with extracorporeal membrane oxygenation (ECMO) support. We aimed to examine the safety of ultra-low-field (ULF; 0.064-T) portable magnetic resonance imaging (pMRI) in patients undergoing ECMO and to investigate the ABI frequency and types with ULF-pMRI.
This was a multicenter prospective observational study (SAFE MRI ECMO study [Assessing the Safety and Feasibility of Bedside Portable Low-Field Brain Magnetic Resonance Imaging in Patients on ECMO]; NCT05469139) from 2 tertiary centers (Johns Hopkins, Baltimore, MD and University of Texas-Houston) with specially trained intensive care units. Primary outcomes were safety of ULF-pMRI during ECMO support, defined as completion of ULF-pMRI without significant adverse events.
Of 53 eligible patients, 3 were not scanned because of a large head size that did not fit within the head coil. ULF-pMRI was performed in 50 patients (median age, 58 years; 52% male), with 34 patients (68%) on venoarterial ECMO and 16 patients (32%) on venovenous ECMO. Of 34 patients on venoarterial ECMO, 11 (22%) were centrally cannulated and 23 (46%) were peripherally cannulated. In venovenous ECMO, 9 (18%) had single-lumen cannulation and 7 (14%) had double-lumen cannulation. Of 50 patients, adverse events occurred in 3 patients (6%), with 2 minor adverse events (ECMO suction event; transient low ECMO flow) and one serious adverse event (intra-aortic balloon pump malfunction attributable to electrocardiographic artifacts). All images demonstrated discernible intracranial pathologies with good quality. ABI was observed in 22 patients (44%). Ischemic stroke (36%) was the most common type of ABI, followed by intracranial hemorrhage (6%) and hypoxic-ischemic brain injury (4%). Of 18 patients (36%) with both ULF-pMRI and head computed tomography within 24 hours, ABI was observed in 9 patients with a total of 10 events (8 ischemic, 2 hemorrhagic events). Of the 8 ischemic events, pMRI observed all 8, and head computed tomography observed only 4 events. For intracranial hemorrhage, pMRI observed only 1 of them, and head computed tomography observed both (2 events).
Our study demonstrates that ULF-pMRI can be performed in patients on ECMO across different ECMO cannulation strategies in specially trained intensive care units. The incidence of ABI was high, seen in 44% of ULF-pMRI studies. ULF-pMRI imaging appears to be more sensitive to ABI, particularly ischemic stroke, compared with head computed tomography.
在床边早期检测急性脑损伤(ABI)对于改善接受体外膜肺氧合(ECMO)支持的患者的生存率至关重要。我们旨在研究超低场(ULF;0.064-T)便携式磁共振成像(pMRI)在接受ECMO治疗的患者中的安全性,并调查ULF-pMRI检测到的ABI频率和类型。
这是一项来自2个三级中心(约翰霍普金斯医院,马里兰州巴尔的摩市和德克萨斯大学休斯顿分校)的多中心前瞻性观察性研究(SAFE MRI ECMO研究[评估床边便携式低场脑磁共振成像在接受ECMO治疗患者中的安全性和可行性];NCT05469139),这些中心设有经过专门培训的重症监护病房。主要结局是ECMO支持期间ULF-pMRI的安全性,定义为完成ULF-pMRI且无重大不良事件。
53例符合条件的患者中,3例因头部尺寸过大无法放入头部线圈而未进行扫描。50例患者接受了ULF-pMRI检查(中位年龄58岁;52%为男性),其中34例(68%)接受静脉-动脉ECMO治疗,16例(32%)接受静脉-静脉ECMO治疗。在接受静脉-动脉ECMO治疗的34例患者中,11例(22%)为中心插管,23例(46%)为外周插管。在静脉-静脉ECMO治疗中,9例(18%)为单腔插管,7例(14%)为双腔插管。50例患者中,3例(6%)发生不良事件,2例为轻微不良事件(ECMO吸引事件;短暂的低ECMO流量),1例为严重不良事件(因心电图伪影导致主动脉内球囊泵故障)。所有图像均显示颅内病变清晰,质量良好。22例(44%)患者观察到ABI。缺血性卒中(36%)是最常见的ABI类型,其次是颅内出血(6%)和缺氧缺血性脑损伤(4%)。在24小时内同时进行ULF-pMRI和头部计算机断层扫描(CT)的18例(36%)患者中,9例患者观察到ABI,共发生10次事件(8次缺血性事件,2次出血性事件)。在8次缺血性事件中,pMRI观察到全部8次,而头部CT仅观察到4次。对于颅内出血,pMRI仅观察到其中1次,而头部CT观察到2次。
我们的研究表明,在经过专门培训的重症监护病房中,不同ECMO插管策略的ECMO患者均可进行ULF-pMRI检查。ABI的发生率较高,在ULF-pMRI研究中为44%。与头部CT相比,ULF-pMRI成像似乎对ABI更敏感,尤其是缺血性卒中。