Akgün Doruk, Gebauer Henry, Paksoy Alp, Eckl Larissa, Hayta Agahan, Ücertas Ata, Barthod-Tonnot Nicolas, Dey Hazra Rony-Orijit, Lacheta Lucca, Moroder Philipp, Pawelke Jonas
Center for Musculoskeletal Surgery, Charité-University Medicine Berlin, Berlin, Germany.
Department of Sports Orthopedics, Technical University of Munich, Munich, Germany.
Orthop J Sports Med. 2024 Nov 14;12(11):23259671241289117. doi: 10.1177/23259671241289117. eCollection 2024 Nov.
Currently, Rockwood type 3 acromioclavicular (AC) joint dislocations are initially treated nonoperatively, whereas surgery is recommended for Rockwood type 5 dislocations. However, multiple studies have been published favoring nonoperative approaches in patients with high-grade Rockwood injuries.
To compare the clinical and radiological outcomes of patients with acute Rockwood type 5 AC joint dislocations treated nonoperatively versus with arthroscopically assisted stabilization.
Cohort study; Level of evidence, 3.
Included were 48 patients with acute Rockwood type 5 dislocation who were initially treated nonoperatively between June 2010 and June 2022 and 48 patients matched according to age, sex, affected side, and follow-up interval who underwent arthroscopically assisted coracoclavicular (CC) stabilization using a suture-button technique, with additional percutaneous AC tape cerclage. Clinical outcomes were assessed based on the Subjective Shoulder Value, Nottingham Clavicle Score, Constant score, and visual analog scale for pain. The radiographic assessment included the CC distance, CC difference ratio, and degree of horizontal instability at final follow-up (62 ± 43 months).
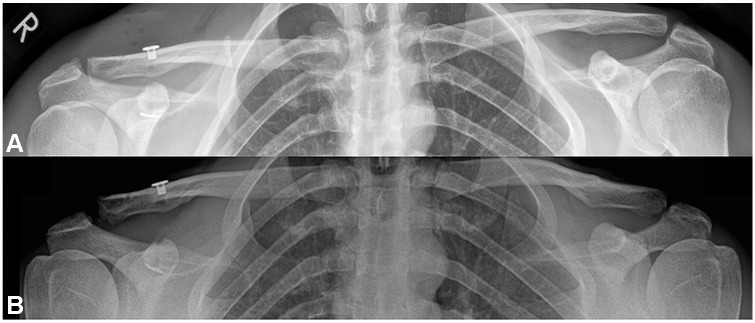
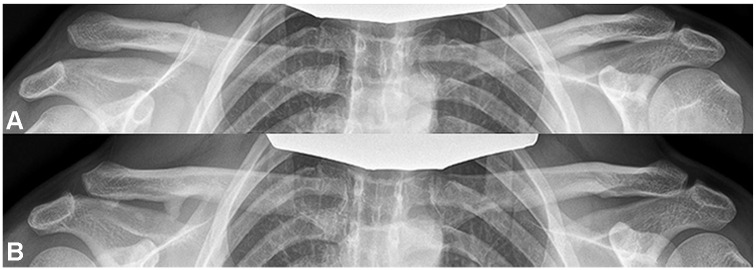
At the final follow-up, the Constant score was significantly higher in the nonoperative group ( = .02). The operative group had significantly higher pain levels on palpation of the AC joint (1.2 ± 2.2 vs 0.19 ± 0.5 for the nonoperative group; = .003). In the operative group, the mean CC difference ratio was significantly higher at the latest follow-up compared with postoperatively (1.3 ± 0.3 vs 0.67 ± 0.3, respectively; < .001), whereas the CC difference ratio of the nonoperative group was significantly reduced at the latest follow-up compared with postinjury (2.0 ± 0.5 vs 2.6 ± 0.8, respectively; < .001). The operative group had a significantly lower CC difference ratio compared with the nonoperative group at final follow-up ( < .001). More than half of the patients (56%) who were treated operatively had a loss of reduction resulting in a Rockwood type 3 state at the latest follow-up, whereas 54% of patients treated nonoperatively had spontaneous reduction of injury severity from Rockwood type 5 to Rockwood type 3.
Although 15% of the nonoperatively treated patients eventually required surgery, successful nonoperative treatment showed similar outcomes to initial operative treatment in patients with acute Rockwood type 5 dislocation.
目前,Rockwood 3型肩锁关节脱位最初采用非手术治疗,而Rockwood 5型脱位则建议手术治疗。然而,已有多项研究支持对Rockwood损伤程度较高的患者采用非手术方法。
比较急性Rockwood 5型肩锁关节脱位患者非手术治疗与关节镜辅助稳定术的临床和影像学结果。
队列研究;证据等级,3级。
纳入2010年6月至2022年6月期间最初接受非手术治疗的48例急性Rockwood 5型脱位患者,以及48例根据年龄、性别、患侧和随访间隔匹配的患者,这些患者采用缝线纽扣技术进行关节镜辅助喙锁(CC)稳定术,并附加经皮肩锁关节胶带环扎术。基于主观肩关节评分、诺丁汉锁骨评分、Constant评分和疼痛视觉模拟量表评估临床结果。影像学评估包括末次随访时(62±43个月)的CC距离、CC差异率和水平不稳定程度。
在末次随访时,非手术组的Constant评分显著更高(P = 0.02)。手术组在触诊肩锁关节时疼痛水平显著更高(手术组为1.2±2.2,非手术组为0.19±0.5;P = 0.003)。在手术组中,与术后相比,最新随访时的平均CC差异率显著更高(分别为1.3±0.3和0.67±0.3;P < 0.001),而非手术组的CC差异率在最新随访时与受伤后相比显著降低(分别为2.0±0.5和2.6±0.8;P < 0.001) 在末次随访时,手术组的CC差异率显著低于非手术组(P < 0.001)。超过一半(56%)接受手术治疗的患者出现复位丢失,在最新随访时导致Rockwood 3型状态,而54%接受非手术治疗的患者损伤严重程度从Rockwood 5型自发减轻至Rockwood 3型。
尽管15%接受非手术治疗的患者最终需要手术,但成功的非手术治疗在急性Rockwood 5型脱位患者中显示出与初始手术治疗相似的结果。