Savige J A, Paspaliaris B, Silvestrini R, Davies D, Nikoloutsopoulos T, Sturgess A, Neil J, Pollock W, Dunster K, Hendle M
University Department of Medicine, Austin and Repatriation Medical Centre, Heidelberg, Victoria, Australia.
J Clin Pathol. 1998 Aug;51(8):568-75. doi: 10.1136/jcp.51.8.568.
To describe the neutrophil fluorescent patterns produced by antineutrophil cytoplasmic antibodies (ANCA) with different antigen specificities, and by other auto- and alloantibodies.
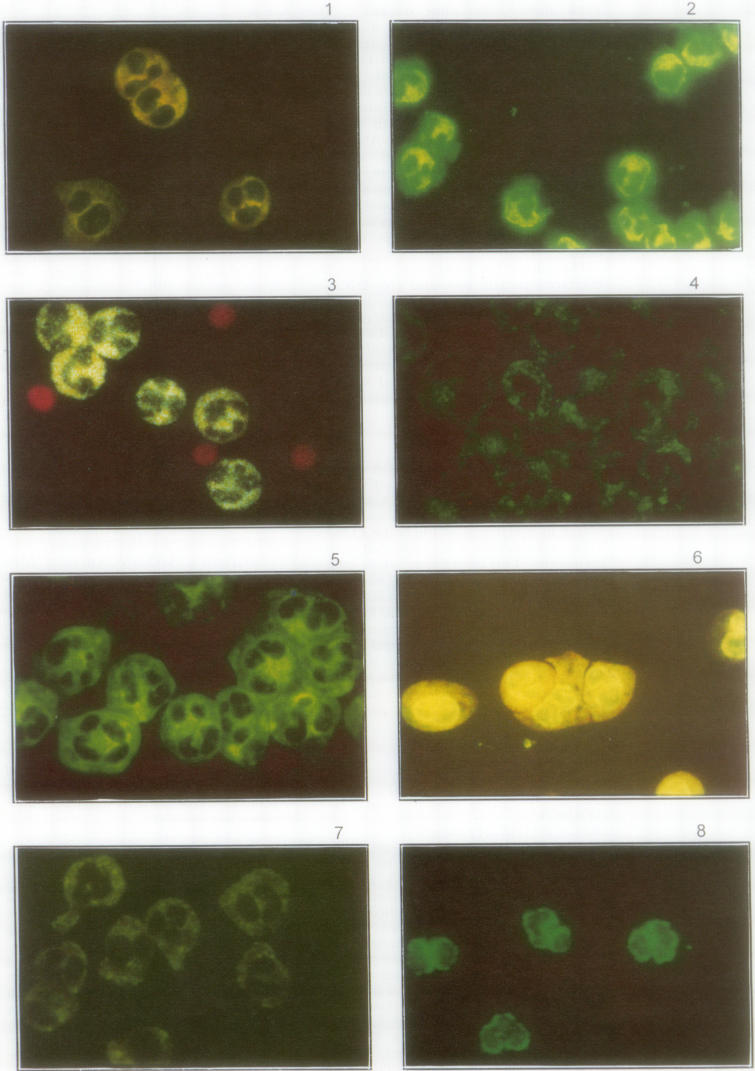
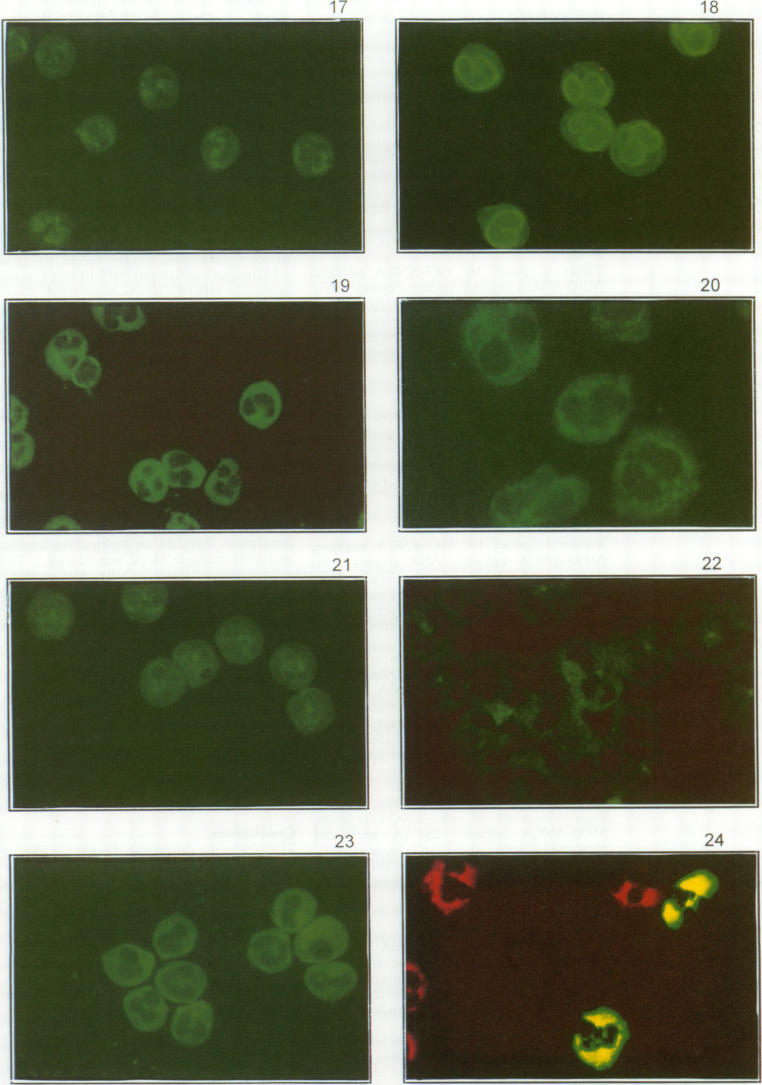
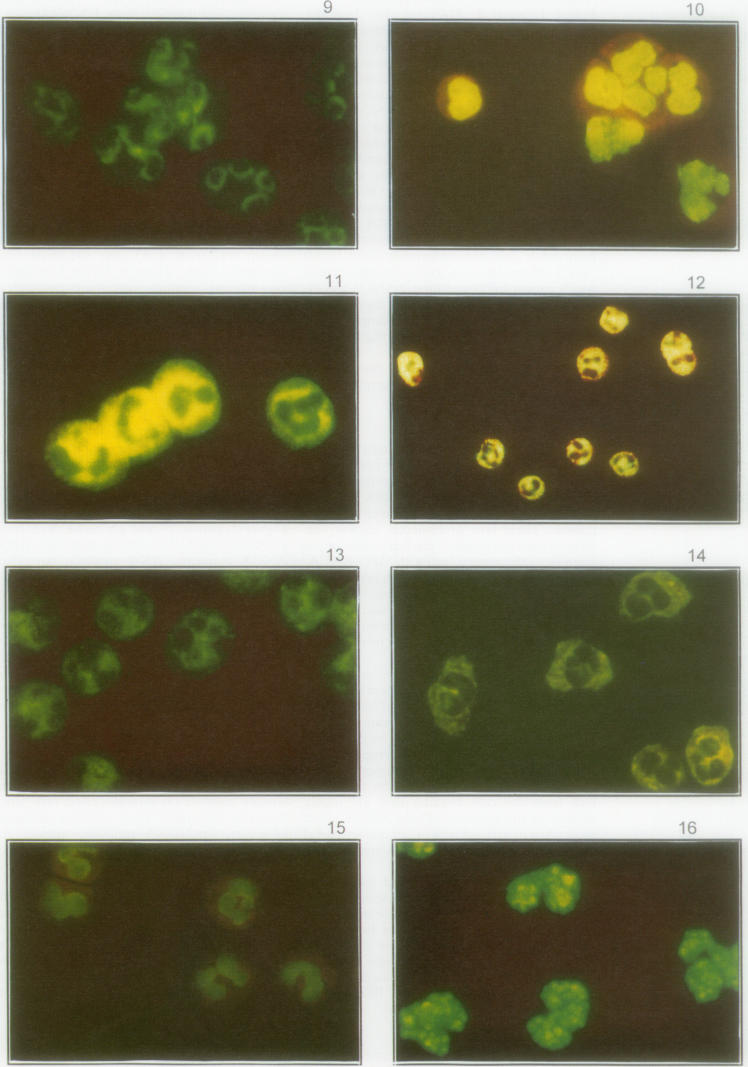
Most sera from patients with active generalised Wegener's granulomatosis result in diffusely granular cytoplasmic neutrophil fluorescence with internuclear accentuation (cANCA) and proteinase 3 (PR3) specificity. About 80% of the sera from patients with microscopic polyangiitis result in perinuclear neutrophil fluorescence with nuclear extension (pANCA) and myeloperoxidase (MPO) specificity, or a cANCA pattern with PR3 specificity. However, many different neutrophil fluorescence patterns are noted on testing for ANCA in routine immunodiagnostic laboratories.
Sera sent for ANCA testing, or containing a variety of auto- and alloantibodies, were studied. They were examined by indirect immunofluorescence according to the recommendations of the first international ANCA workshop, and for PR3 and MPO specificity in commercial and in-house enzyme linked immunosorbent assays (ELISA).
Sera with typical cANCA accounted for only half of all neutrophil cytoplasmic fluorescence. Other sera had "flatter" fluorescence without internuclear accentuation, and the corresponding antigens included MPO and bactericidal/permeability increasing protein (BPI), but were usually unknown. Peripheral nuclear fluorescence without nuclear extension occurred typically when the antigens were BPI, lactoferrin, lysozyme, elastase, or cathepsin G. Most types of ANA were evident on ethanol fixed neutrophil nuclei. AntidsDNA, antiRo, and antilamin antibodies resembled pANCA. Antimicrobial and antiribosomal antibodies produced cytoplasmic fluorescence, and antiGolgi antibodies, a pANCA. Sera from patients with anti-smooth muscle antibodies were associated with cytoplasmic fluorescence. There was no neutrophil fluorescence with anti-skeletal muscle and anti-heart muscle antibodies, anti-liver/kidney microsomal, antithyroid microsomal, or antiadrenal antibodies. Alloantibodies such as antiNB1 typically resulted in cytoplasmic fluorescence of only a subpopulation of the neutrophils.
The ability to distinguish between different neutrophil fluorescence patterns, and the patterns seen with other auto- and alloantibodies is helpful diagnostically. However, the demonstration of MPO or PR3 specificity by ELISA will indicate that the neutrophil fluorescence is probably clinically significant, and that the diagnosis is likely to be Wegener's granulomatosis or microscopic polyangiitis.
描述具有不同抗原特异性的抗中性粒细胞胞浆抗体(ANCA)以及其他自身抗体和同种抗体所产生的中性粒细胞荧光模式。
大多数活动性全身性韦格纳肉芽肿患者的血清会导致中性粒细胞胞浆出现弥漫性颗粒状荧光且核间增强(cANCA),并具有蛋白酶3(PR3)特异性。约80%显微镜下多血管炎患者的血清会导致中性粒细胞核周荧光且核延伸(pANCA),并具有髓过氧化物酶(MPO)特异性,或出现具有PR3特异性的cANCA模式。然而,在常规免疫诊断实验室检测ANCA时会发现许多不同的中性粒细胞荧光模式。
研究送检进行ANCA检测的血清,或含有多种自身抗体和同种抗体的血清。根据第一届国际ANCA研讨会的建议,通过间接免疫荧光对其进行检测,并在商业和内部酶联免疫吸附测定(ELISA)中检测PR3和MPO特异性。
具有典型cANCA的血清仅占所有中性粒细胞胞浆荧光的一半。其他血清具有“较平”的荧光且无核间增强,相应抗原包括MPO和杀菌/通透性增加蛋白(BPI),但通常未知。当抗原为BPI、乳铁蛋白、溶菌酶、弹性蛋白酶或组织蛋白酶G时,通常会出现无核延伸的核周荧光。大多数类型的抗核抗体在乙醇固定的中性粒细胞核上很明显。抗双链DNA、抗Ro和抗层粘连蛋白抗体类似pANCA。抗菌和抗核糖体抗体产生胞浆荧光,抗高尔基体抗体产生pANCA。抗平滑肌抗体患者的血清与胞浆荧光有关。抗骨骼肌和抗心肌抗体、抗肝/肾微粒体抗体、抗甲状腺微粒体抗体或抗肾上腺抗体未出现中性粒细胞荧光。诸如抗NB1等同种抗体通常仅导致中性粒细胞亚群出现胞浆荧光。
区分不同的中性粒细胞荧光模式以及其他自身抗体和同种抗体所呈现的模式在诊断上是有帮助的。然而,通过ELISA证明MPO或PR3特异性将表明中性粒细胞荧光可能具有临床意义,且诊断可能为韦格纳肉芽肿或显微镜下多血管炎。