Starkiene Liudvika, Smigelskas Kastytis, Padaiga Zilvinas, Reamy Jack
Department of Preventive Medicine, Kaunas University of Medicine, Mickeviciaus str. 9, LT-44307 Kaunas, Lithuania.
BMC Fam Pract. 2005 Oct 4;6:41. doi: 10.1186/1471-2296-6-41.
When health care reform was started in 1991, the physician workforce in Lithuania was dominated by specialists, and the specialty of family physician (FP) did not exist at all. During fifteen years of Lithuania's independence this specialty evolved rapidly and over 1,900 FPs were trained or retrained. Since 2003, the Lithuanian health care sector has undergone restructuring to optimize the network of health care institutions as well as the delivery of services; specific attention has been paid to the development of services provided by FPs, with more health care services shifted from the hospital level to the primary health care level. In this paper we analyze if an adequate workforce of FPs will be available in the future to take over new emerging tasks.
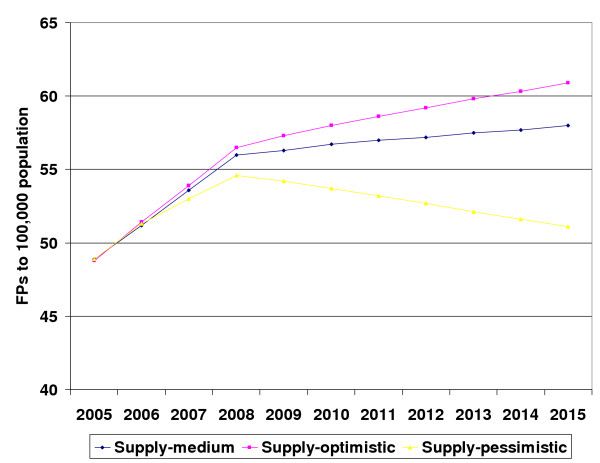
A computer spreadsheet simulation model was used to project the supply of FPs in 2006-2015. The supply was projected according to three scenarios, which took into account different rates of retirement, migration and drop out from training. In addition different population projections and enrollment numbers in residency programs were also considered. Three requirement scenarios were made using different approaches. In the first scenario we used the requirement estimated by a panel of experts using the Delphi technique. The second scenario was based on the number of visits to FPs in 2003 and took into account the goal to increase the number of visits. The third scenario was based on the determination that one FP should serve no more than 2,000 inhabitants. The three scenarios for the projection of supply were compared with the three requirement scenarios.
The supply of family physicians will be higher in 2015 compared to 2005 according to all projection scenarios. The largest differences in the supply scenarios were caused by different migration rates, enrollment numbers to training programs and the retirement age. The second supply scenario, which took into account 1.1% annual migration rate, stable enrollment to residency programs and later retirement, appears to be the most probable. The first requirement scenario, which was based on the opinion of well-informed key experts in the field, appears to be the best reflection of FP requirements; however none of the supply scenarios considered would satisfy these requirements.
Despite the rapid expansion of the FP workforce during the last fifteen years, ten-year forecasts of supply and requirement indicate that the number of FPs in 2015 will not be sufficient. The annual enrollment in residency training programs should be increased by at least 20% for the next three years. Accurate year-by-year monitoring of the workforce is crucial in order to prevent future shortages and to maintain the desired family physician workforce.
1991年医疗改革启动时,立陶宛的医师队伍以专科医生为主,家庭医生这一专业根本不存在。在立陶宛独立的15年里,这一专业迅速发展,1900多名家庭医生接受了培训或再培训。自2003年以来,立陶宛医疗部门进行了重组,以优化医疗机构网络和服务提供;特别关注家庭医生提供的服务发展,更多的医疗服务从医院层面转移到了初级医疗层面。在本文中,我们分析未来是否会有足够的家庭医生队伍来承担新出现的任务。
使用计算机电子表格模拟模型预测2006 - 2015年家庭医生的供应情况。根据三种情景预测供应情况,这三种情景考虑了不同的退休率、移民率和培训辍学率。此外,还考虑了不同的人口预测和住院医师培训项目的招生人数。使用不同方法制定了三种需求情景。在第一种情景中,我们使用专家小组采用德尔菲技术估计的需求。第二种情景基于2003年家庭医生的就诊人数,并考虑了增加就诊人数的目标。第三种情景基于确定一名家庭医生服务的居民人数不应超过2000人。将三种供应预测情景与三种需求情景进行比较。
根据所有预测情景,2015年家庭医生的供应量将高于2005年。供应情景中最大的差异是由不同的移民率、培训项目的招生人数和退休年龄造成的。第二种供应情景,即考虑到每年1.1%的移民率、住院医师培训项目稳定的招生人数和较晚的退休年龄,似乎是最有可能的。第一种需求情景基于该领域消息灵通的关键专家的意见,似乎最能反映家庭医生的需求;然而,所考虑的任何供应情景都无法满足这些需求。
尽管在过去15年里家庭医生队伍迅速扩大,但供应和需求的十年预测表明,2015年家庭医生的数量将不足。未来三年住院医师培训项目的年度招生人数应至少增加
20%。对劳动力进行准确的逐年监测对于防止未来短缺和维持理想的家庭医生队伍至关重要。