University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA.
Environ Health Perspect. 2010 Sep;118(9):1189-95. doi: 10.1289/ehp.0901220. Epub 2010 Apr 8.
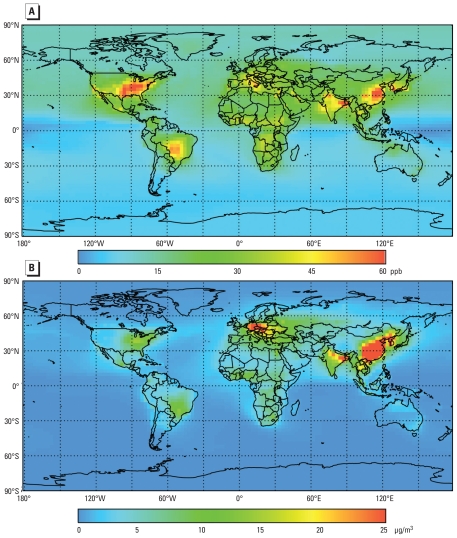
Ground-level concentrations of ozone (O3) and fine particulate matter [< or = 2.5 microm in aerodynamic diameter (PM2.5)] have increased since preindustrial times in urban and rural regions and are associated with cardiovascular and respiratory mortality.
We estimated the global burden of mortality due to O3 and PM2.5 from anthropogenic emissions using global atmospheric chemical transport model simulations of preindustrial and present-day (2000) concentrations to derive exposure estimates.
Attributable mortalities were estimated using health impact functions based on long-term relative risk estimates for O3 and PM2.5 from the epidemiology literature. Using simulated concentrations rather than previous methods based on measurements allows the inclusion of rural areas where measurements are often unavailable and avoids making assumptions for background air pollution.
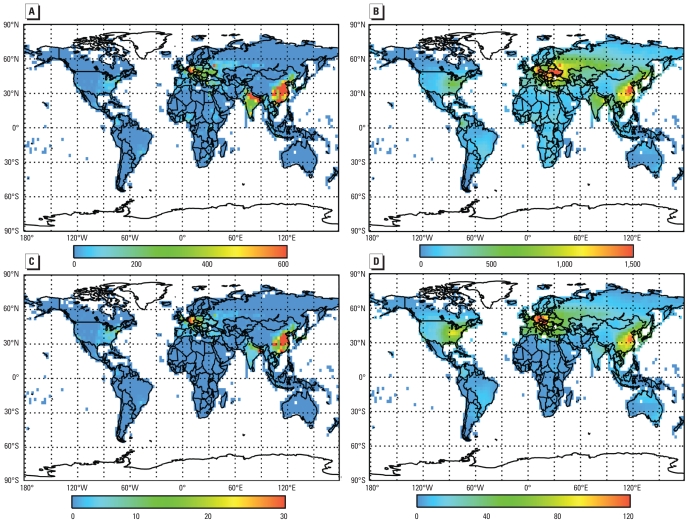
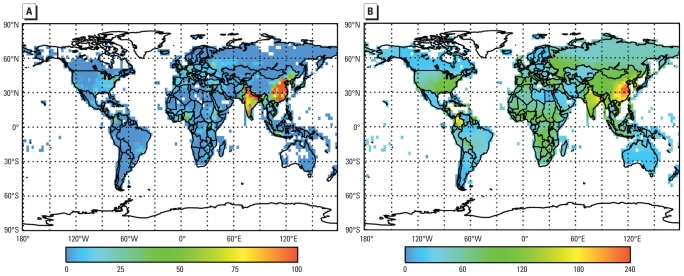
Anthropogenic O3 was associated with an estimated 0.7 +/- 0.3 million respiratory mortalities (6.3 +/- 3.0 million years of life lost) annually. Anthropogenic PM2.5 was associated with 3.5 +/- 0.9 million cardiopulmonary and 220,000 +/- 80,000 lung cancer mortalities (30 +/- 7.6 million years of life lost) annually. Mortality estimates were reduced approximately 30% when we assumed low-concentration thresholds of 33.3 ppb for O3 and 5.8 microg/m3 for PM2.5. These estimates were sensitive to concentration thresholds and concentration-mortality relationships, often by > 50%.
Anthropogenic O3 and PM2.5 contribute substantially to global premature mortality. PM2.5 mortality estimates are about 50% higher than previous measurement-based estimates based on common assumptions, mainly because of methodologic differences. Specifically, we included rural populations, suggesting higher estimates; however, the coarse resolution of the global atmospheric model may underestimate urban PM(2.5) exposures.
自工业化前时期以来,城市和农村地区的地面臭氧(O3)和细颗粒物(<或= 2.5 微米空气动力学直径的 PM2.5)浓度不断增加,与心血管和呼吸道死亡率有关。
我们使用全球大气化学输送模型模拟工业化前和现在(2000 年)的浓度,估算人为排放源引起的 O3 和 PM2.5 造成的全球死亡率负担,从而得出暴露量估算值。
根据流行病学文献中 O3 和 PM2.5 的长期相对风险估计值,利用健康影响函数估算可归因的死亡率。与之前基于测量值的方法(该方法常常无法测量农村地区的浓度,并且需要对背景空气污染做出假设)不同,本研究使用模拟浓度可以将农村地区也包括在内,从而避免做出假设。
人为 O3 每年与约 0.7 +/- 0.3 百万例呼吸道死亡(6.3 +/- 3.0 百万年生命损失)相关。人为 PM2.5 每年与 3.5 +/- 0.9 百万例心肺疾病和 220,000 +/- 80,000 例肺癌死亡相关(30 +/- 7.6 百万年生命损失)。当我们假设 O3 的低浓度阈值为 33.3 ppb 和 PM2.5 的浓度阈值为 5.8 microg/m3 时,死亡率估计值降低了约 30%。这些估计值对浓度阈值和浓度-死亡率关系很敏感,变化幅度常常超过 50%。
人为 O3 和 PM2.5 是导致全球过早死亡的主要原因。PM2.5 的死亡率估计值比之前基于常见假设的基于测量的估计值高约 50%,主要是因为方法学上的差异。具体而言,我们将农村人口包括在内,表明估计值更高;但是,全球大气模型的粗糙分辨率可能低估了城市 PM(2.5)暴露量。