Clinica Malattie Infettive, AOU San Martino, L.go R.Benzi 10, 16132 Genova, Italy.
Crit Care. 2010;14(6):244. doi: 10.1186/cc9239. Epub 2010 Dec 1.
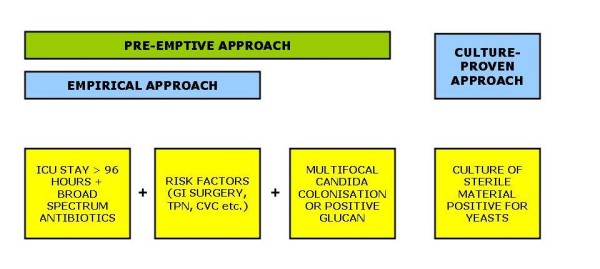
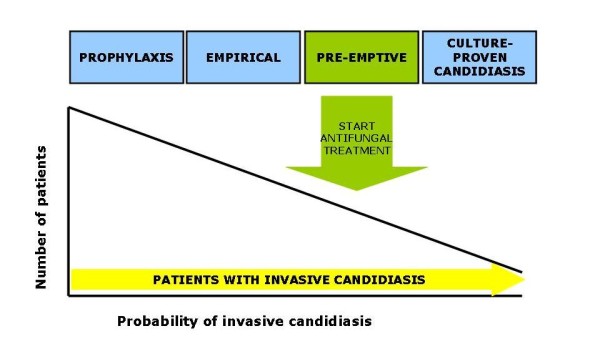
Candida is one of the most frequent pathogens in bloodstream infections, and is associated with significant morbidity and mortality. The epidemiology of species responsible for invasive candidiasis, both at local and worldwide levels, has been changing - shifting from Candida albicans to non-albicans species, which can be resistant to fluconazole (Candida krusei and Candida glabrata) or difficult to eradicate because of biofilm production (Candida parapsilosis). Numerous intensive care unit patients have multiple risk factors for developing this infection, which include prolonged hospitalisation, use of broad-spectrum antibiotics, presence of intravascular catheters, parenteral nutrition, high Acute Physiology and Chronic Health Evaluation score, and so forth. Moreover, delaying the specific therapy was shown to further increase morbidity and mortality. To minimise the impact of this infection, several management strategies have been developed - prophylaxis, empirical therapy, pre-emptive therapy and culture-based treatment. Compared with prophylaxis, empirical and pre-emptive approaches allow one to reduce the exposure to antifungals by targeting only the patients at high risk of candidemia, without delaying therapy until the moment blood Candida is identified in blood cultures. The agents recommended for initial treatment of candidemia in critically ill patients include echinocandins and lipid formulation of amphotericin B.
念珠菌是血流感染中最常见的病原体之一,与较高的发病率和死亡率相关。引起侵袭性念珠菌病的病原菌在局部和全球范围内的流行病学特征一直在发生变化——从白念珠菌向非白念珠菌转变,后者可能对氟康唑耐药(克柔念珠菌和光滑念珠菌),或者由于生物膜的产生而难以根除(近平滑念珠菌)。许多重症监护病房患者存在发生这种感染的多种危险因素,包括长时间住院、广谱抗生素的使用、血管内导管的存在、肠外营养、高急性生理学和慢性健康评估评分等。此外,延迟特定治疗会进一步增加发病率和死亡率。为了尽量减少这种感染的影响,已经制定了几种管理策略——预防、经验性治疗、抢先治疗和基于培养的治疗。与预防相比,经验性和抢先治疗方法允许仅针对有发生念珠菌血症高风险的患者进行治疗,从而减少抗真菌药物的暴露,而无需等到血培养中发现血液念珠菌时才开始治疗。推荐用于重症患者初始治疗的药物包括棘白菌素类和两性霉素 B 脂质体。