Department of Infectious Diseases, Ryhov County Hospital, Jönköping, Sweden.
J Neuroinflammation. 2011 Apr 20;8:36. doi: 10.1186/1742-2094-8-36.
Previous studies indicate that successful resolution of Lyme neuroborreliosis (NB) is associated with a strong T helper (Th) 1-type cytokine response in the cerebrospinal fluid (CSF) followed by a down-regulating Th2 response, whereas the role of the recently discovered Th17 cytokine response is unknown.
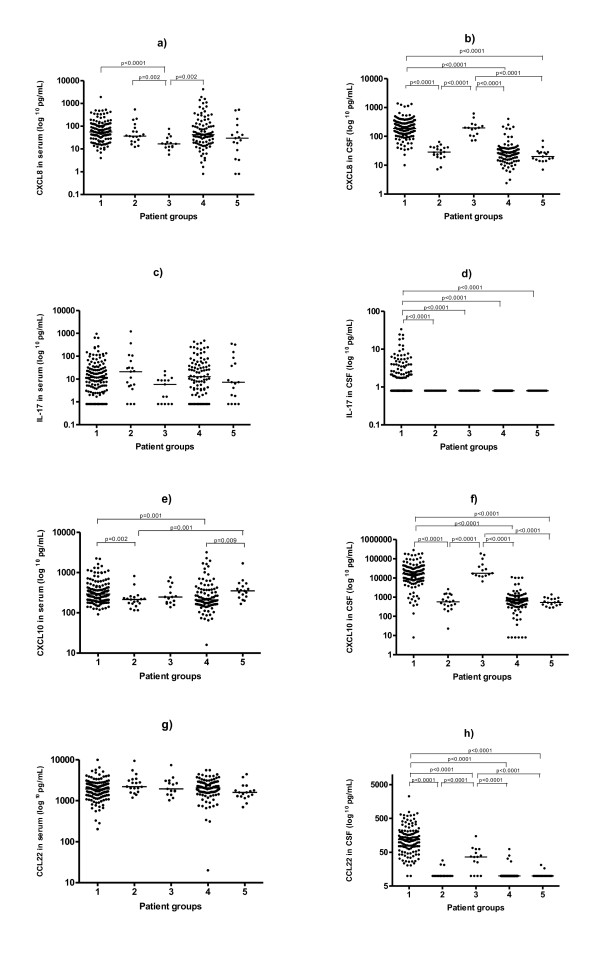
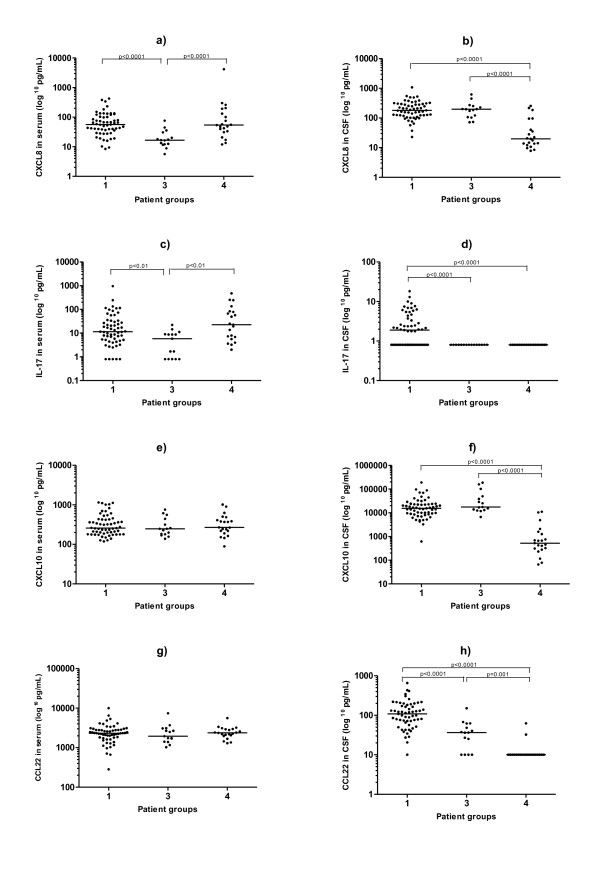
To investigate the relative contribution of different Th associated cytokine/chemokine responses, we used a multiple bead array to measure the levels of CXCL10 (Th1 marker), CCL22 (Th2 marker), IL-17 (Th17 marker) and CXCL8 (general inflammation marker), in serum and in CSF from untreated patients with confirmed NB (n = 133), and non-NB patients (n = 96), and related the findings to clinical data. Samples from patients with possible early NB (n = 15) and possible late NB (n = 19) were also analysed, as well as samples from an additional control group with orthopaedic patients (n = 17), where CSF was obtained at spinal anaesthesia.
The most prominent differences across groups were found in the CSF. IL-17 was elevated in CSF in 49% of the patients with confirmed NB, but was not detectable in the other groups. Patients with confirmed NB and possible early NB had significantly higher CSF levels of CXCL10, CCL22 and CXCL8 compared to both the non-NB group and the control group (p < 0.0001 for all comparisons). Patients in the early NB group, showing a short duration of symptoms, had lower CCL22 levels in CSF than did the confirmed NB group (p < 0.0001). Furthermore, patients within the confirmed NB group showing a duration of symptoms <2 weeks, tended to have lower CCL22 levels in CSF than did those with longer symptom duration (p = 0.023). Cytokine/chemokine levels were not correlated with clinical parameters or to levels of anti-Borrelia-antibodies.
Our results support the notion that early NB is dominated by a Th1-type response, eventually accompanied by a Th2 response. Interestingly, IL-17 was increased exclusively in CSF from patients with confirmed NB, suggesting a hitherto unknown role for Th17 in NB. However, for conclusive evidence, future prospective studies are needed.
先前的研究表明,成功解决莱姆神经Borreliosis(NB)与脑脊液(CSF)中强烈的辅助性 T 细胞(Th)1 型细胞因子反应有关,随后是下调的 Th2 反应,而最近发现的 Th17 细胞因子反应的作用尚不清楚。
为了研究不同的 Th 相关细胞因子/趋化因子反应的相对贡献,我们使用多重珠阵列来测量未经治疗的确诊 NB 患者(n = 133)和非 NB 患者(n = 96)的血清和 CSF 中的 CXCL10(Th1 标志物)、CCL22(Th2 标志物)、IL-17(Th17 标志物)和 CXCL8(一般炎症标志物)水平,并将这些发现与临床数据相关联。还分析了可能早期 NB(n = 15)和可能晚期 NB(n = 19)患者的样本,以及来自接受骨科手术患者的额外对照组的样本(n = 17),其中在脊髓麻醉时获得 CSF。
各组之间最明显的差异出现在 CSF 中。在确诊的 NB 患者中,49%的患者 CSF 中 IL-17 升高,但在其他组中未检测到。与非 NB 组和对照组相比,确诊的 NB 和可能早期 NB 患者的 CSF 中 CXCL10、CCL22 和 CXCL8 水平明显更高(所有比较 p < 0.0001)。症状持续时间较短的早期 NB 组患者 CSF 中的 CCL22 水平低于确诊的 NB 组(p < 0.0001)。此外,在确诊的 NB 组中,症状持续时间<2 周的患者 CSF 中的 CCL22 水平低于症状持续时间较长的患者(p = 0.023)。细胞因子/趋化因子水平与临床参数或抗 Borrelia 抗体水平均无相关性。
我们的结果支持早期 NB 主要由 Th1 型反应主导的观点,最终伴有 Th2 反应。有趣的是,IL-17 仅在确诊的 NB 患者的 CSF 中增加,提示 Th17 在 NB 中具有未知的作用。然而,为了得出确凿的证据,需要进行未来的前瞻性研究。