Smith Zachary A, Li Zhenzhou, Raphael Dan, Khoo Larry T
Division of Neurosurgery, The Spine Clinic of Los Angeles, Good Samaritan Hospital, Los Angeles, CA 90017, USA.
Surg Neurol Int. 2011;2:129. doi: 10.4103/2152-7806.85469. Epub 2011 Sep 27.
Perineural cysts of the sacrum, or Tarlov cysts, are cerebrospinal fluid (CSF)-filled sacs that commonly occur at the intersection of the dorsal root ganglion and posterior nerve root in the lumbosacral spine. Although often asymptomatic, these cysts have the potential to produce significant symptoms, including pain, weakness, and/or bowel or bladder incontinence. We present a case in which the sacral roof is removed and reconstructed via plated laminoplasty and describe how this technique could be of potential use in maximizing outcomes.
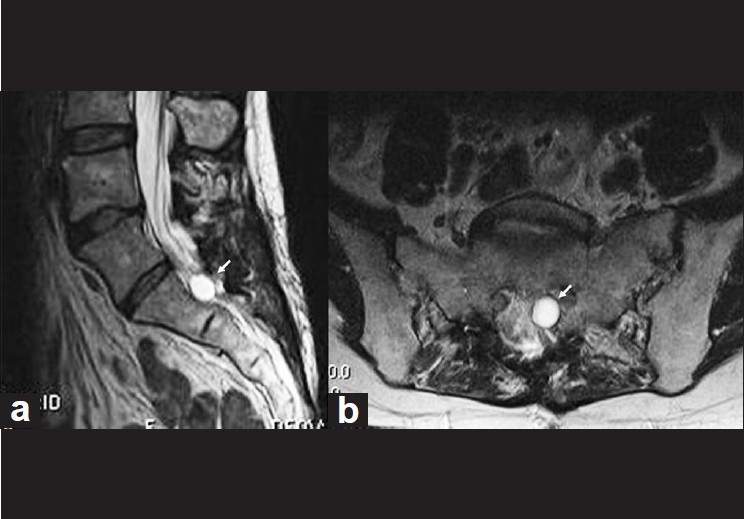
We describe technical aspects of a sacral laminoplasty in conjunction with cyst fenestration for a symptomatic sacral perineural cyst in a 50-year-old female with severe sacral pain, lumbosacral radiculopathy, and progressive incontinence. This patient had magnetic resonance imaging (MRI) and computed tomography (CT)-myelographic evidence of a non-filling, 1.7 × 1.4 cm perineural cyst that was causing significant compression of the cauda equina and sacral nerve roots. This surgical technique was also employed in a total of 18 patients for symptomatic tarlov cysts with their radiographic and clinical results followed in a prospective fashion.
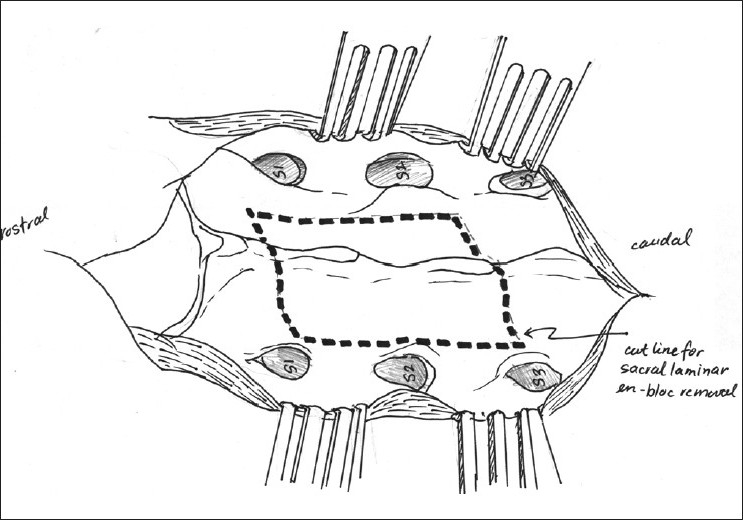
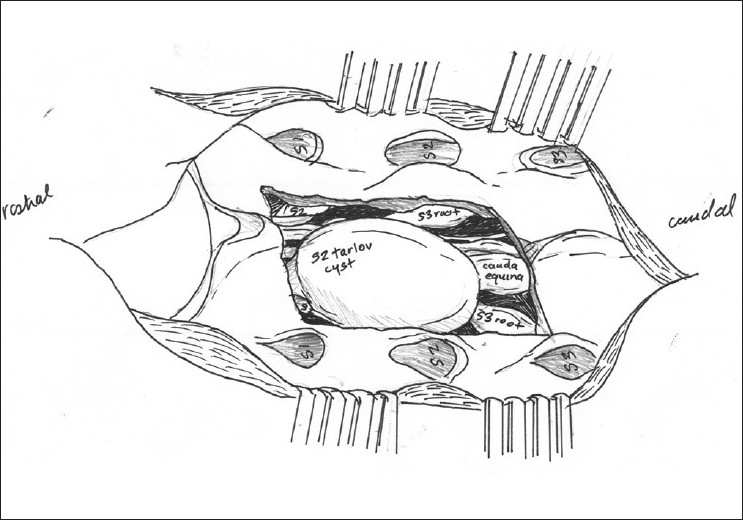
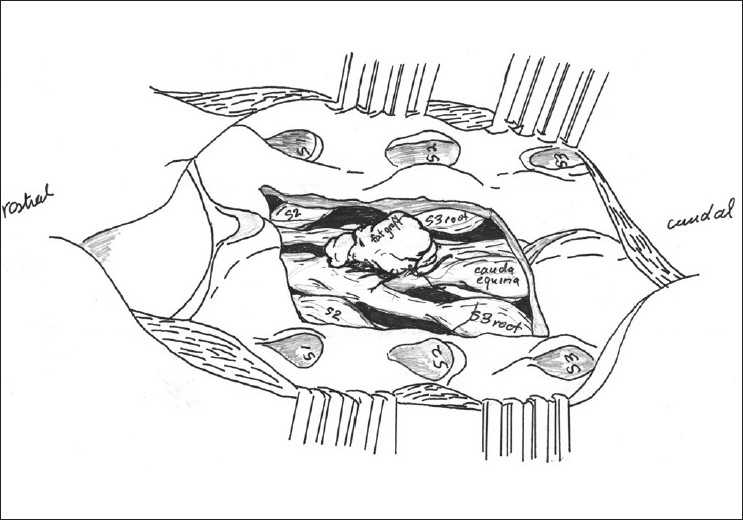
Intraoperative images, drawings, and video are presented to demonstrate both the technical aspects of this technique and the regional anatomy. Postoperative MRI scan demonstrated complete removal of the Tarlov cyst. The patient's symptoms improved dramatically and she regained normal bladder function. There was no evidence of radiographic recurrence at 12 months. At an average 16 month followup interval 10/18 patients had significant relief with mild or no residual complaints, 3/18 reported relief but had persistent coccydynia around the surgical area, 2/18 had primary relief but developed new low back pain and/or lumbar radiculopathy, 2/18 remained at their preoperative level of symptoms, and 1/18 had relief of their preoperative leg pain but developed new pain and neurological deficits.
Sacral laminoplasty and microscopic cystic fenestration is a feasible approach in the operative treatment of this difficult, and often controversial, spinal pathology. This technique may be used further and studied in an attempt to minimize potential surgical morbidity, including CSF leaks, cyst recurrence, and sacral insufficiency fractures.
骶骨神经周围囊肿,即塔尔洛夫囊肿,是充满脑脊液(CSF)的囊袋,通常发生于腰骶部脊柱背根神经节与后神经根的交汇处。尽管这些囊肿通常无症状,但有可能产生严重症状,包括疼痛、无力和/或大小便失禁。我们报告一例通过钢板辅助椎板成形术切除并重建骶骨顶的病例,并描述该技术如何可能有助于实现最佳治疗效果。
我们描述了一名50岁女性有严重骶骨疼痛、腰骶神经根病和进行性大小便失禁的有症状骶骨神经周围囊肿行骶骨椎板成形术联合囊肿开窗术的技术细节。该患者的磁共振成像(MRI)和计算机断层扫描(CT)脊髓造影显示有一个1.7×1.4 cm的未充盈神经周围囊肿,对马尾和骶神经根造成明显压迫。该手术技术还应用于另外18例有症状的塔尔洛夫囊肿患者,并对其影像学和临床结果进行了前瞻性随访。
展示了术中图像、绘图和视频,以说明该技术的技术细节和局部解剖结构。术后MRI扫描显示塔尔洛夫囊肿已完全切除。患者症状显著改善,恢复了正常膀胱功能。12个月时无影像学复发迹象。在平均16个月的随访期内,18例患者中有10例症状明显缓解,仅有轻微或无残留不适;3/18报告症状缓解,但手术区域周围仍有持续性尾骨痛;2/18最初症状缓解,但出现了新的下腰痛和/或腰神经根病;2/18症状仍维持在术前水平;1/18术前腿痛缓解,但出现了新的疼痛和神经功能缺损。
骶骨椎板成形术和显微镜下囊肿开窗术是治疗这种棘手且常具争议性的脊柱病变的一种可行方法。该技术可进一步应用并开展研究,以尽量减少潜在的手术并发症,包括脑脊液漏、囊肿复发和骶骨不全骨折。