Center for Global Health, Department of Internal Medicine, University of New Mexico Health Sciences Center, Albuquerque NM, USA.
Int J Biol Sci. 2011;7(9):1427-42. doi: 10.7150/ijbs.7.1427. Epub 2011 Nov 2.
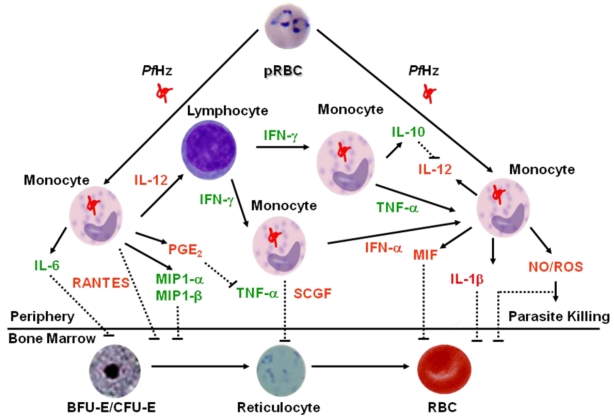
Greater than 80% of malaria-related mortality occurs in sub-Saharan Africa due to infections with Plasmodium falciparum. The majority of P. falciparum-related mortality occurs in immune-naïve infants and young children, accounting for 18% of all deaths before five years of age. Clinical manifestations of severe falciparum malaria vary according to transmission intensity and typically present as one or more life-threatening complications, including: hyperparasitemia; hypoglycemia; cerebral malaria; severe malarial anemia (SMA); and respiratory distress. In holoendemic transmission areas, SMA is the primary clinical manifestation of severe childhood malaria, with cerebral malaria occurring only in rare cases. Mortality rates from SMA can exceed 30% in pediatric populations residing in holoendemic transmission areas. Since the vast majority of the morbidity and mortality occurs in immune-naïve African children less than five years of age, with SMA as the primary manifestation of severe disease, this review will focus primarily on the innate immune mechanisms that govern malaria pathogenesis in this group of individuals. The pathophysiological processes that contribute to SMA involve direct and indirect destruction of parasitized and non-parasitized red blood cells (RBCs), inefficient and/or suppression of erythropoiesis, and dyserythropoiesis. While all of these causal etiologies may contribute to reduced hemoglobin (Hb) concentrations in malaria-infected individuals, data from our laboratory and others suggest that SMA in immune-naïve children is characterized by a reduced erythropoietic response. One important cause of impaired erythroid responses in children with SMA is dysregulation in the innate immune response. Phagocytosis of malarial pigment hemozoin (Hz) by monocytes, macrophages, and neutrophils is a central factor for promoting dysregulation in innate inflammatory mediators. As such, the role of P. falciparum-derived Hz (PfHz) in mediating suppression of erythropoiesis through its ability to cause dysregulation in pro- and anti-inflammatory cytokines, growth factors, chemokines, and effector molecules is discussed in detail. An improved understanding of the etiological basis of suppression of erythropoietic responses in children with SMA may offer the much needed therapeutic alternatives for control of this global disease burden.
由于感染疟原虫(Plasmodium falciparum),超过 80%的疟疾相关死亡发生在撒哈拉以南非洲地区。大多数与疟原虫相关的死亡发生在免疫初发的婴儿和幼儿中,占五岁以下所有死亡人数的 18%。严重疟疾的临床表现因传播强度而异,通常表现为一种或多种危及生命的并发症,包括:高寄生虫血症;低血糖;脑型疟疾;严重疟疾贫血(SMA);呼吸窘迫。在全疫源传播地区,SMA 是严重儿童疟疾的主要临床表现,脑型疟疾仅在极少数情况下发生。居住在全疫源传播地区的儿科人群中,SMA 的死亡率可超过 30%。由于绝大多数发病率和死亡率发生在免疫初发的五岁以下非洲儿童中,且 SMA 是严重疾病的主要表现,因此本综述将主要关注控制该组人群中疟疾发病机制的固有免疫机制。导致 SMA 的病理生理过程涉及寄生和非寄生红细胞(RBC)的直接和间接破坏、红细胞生成效率降低和/或受抑制,以及红细胞生成异常。虽然所有这些因果病因都可能导致疟疾感染个体的血红蛋白(Hb)浓度降低,但我们实验室和其他实验室的数据表明,免疫初发儿童中的 SMA 表现为红细胞生成反应降低。SMA 患儿红细胞生成反应受损的一个重要原因是固有免疫反应失调。单核细胞、巨噬细胞和中性粒细胞吞噬疟原虫色素血褐素(Hz)是促进固有炎症介质失调的核心因素。因此,详细讨论了疟原虫衍生的 Hz(PfHz)通过引起促炎和抗炎细胞因子、生长因子、趋化因子和效应分子的失调,在介导红细胞生成抑制中的作用。对 SMA 患儿红细胞生成反应抑制的病因学基础有了更好的理解,可能为控制这一全球疾病负担提供急需的治疗选择。