Institute of Cancer Research, London, UK.
Trials. 2012 Nov 29;13:228. doi: 10.1186/1745-6215-13-228.
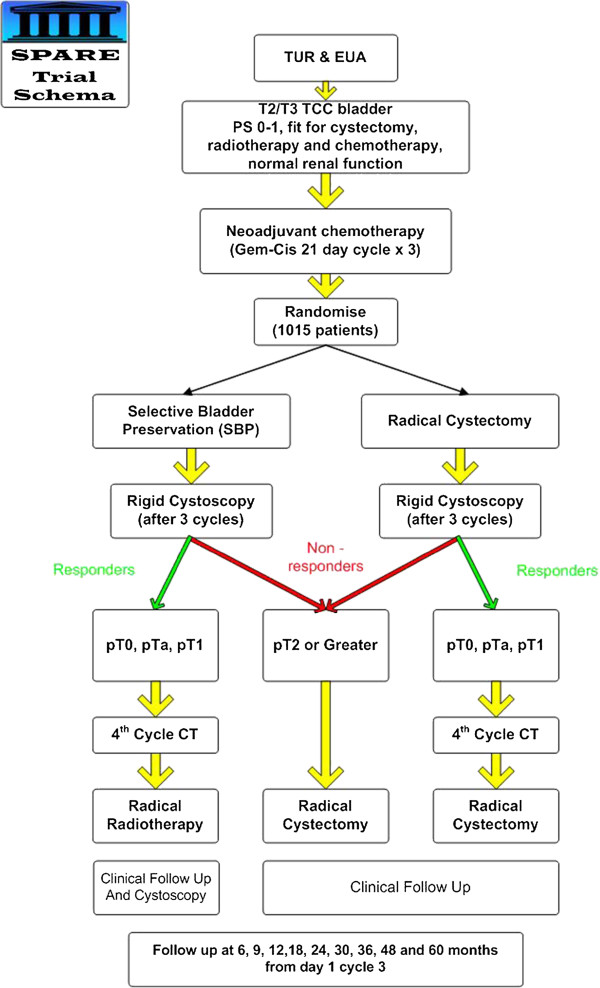
Evidence suggests that poor recruitment into clinical trials rests on a patient 'deficit' model - an inability to comprehend trial processes. Poor communication has also been cited as a possible barrier to recruitment. A qualitative patient interview study was included within the feasibility stage of a phase III non-inferiority Randomized Controlled Trial (RCT) (SPARE, CRUK/07/011) in muscle invasive bladder cancer. The aim was to illuminate problems in the context of randomization.
The qualitative study used a 'Framework Analysis' that included 'constant comparison' in which semi-structured interviews are transcribed, analyzed, compared and contrasted both between and within transcripts. Three researchers coded and interpreted data.
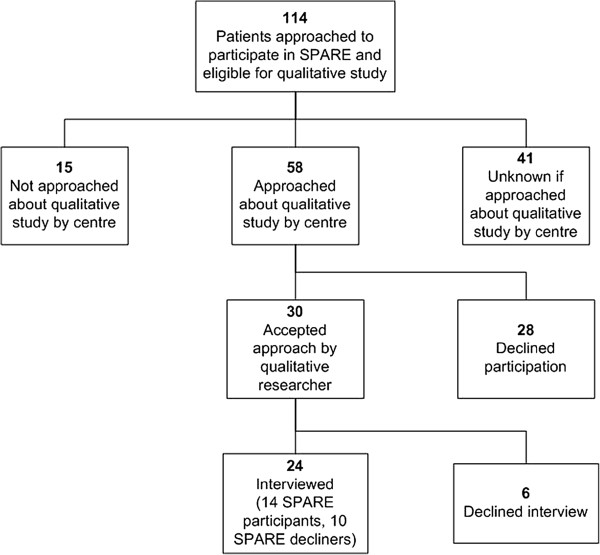
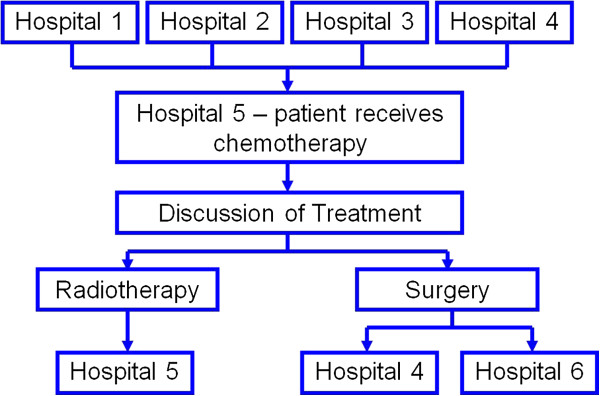
Twenty-four patients agreed to enter the interview study; 10 decliners of randomization and 14 accepters, of whom 2 subsequently declined their allocated treatment.The main theme applying to the majority of the sample was confusion and ambiguity. There was little indication that confusion directly impacted on decisions to enter the SPARE trial. However, confusion did appear to impact on ethical considerations surrounding 'informed consent', as well as cause a sense of alienation between patients and health personnel.Sub-optimal communication in many guises accounted for the confusion, together with the logistical elements of a trial that involved treatment options delivered in a number of geographical locations.
These data highlight the difficulty of providing balanced and clear trial information within the UK health system, despite best intentions. Involvement of multiple professionals can impact on communication processes with patients who are considering participation in RCTs. Our results led us to question the 'deficit' model of patient behavior. It is suggested that health professionals might consider facilitating a context in which patients feel fully included in the trial enterprise and potentially consider alternatives to randomization where complex interventions are being tested.
ISRCTN61126465.
有证据表明,临床试验的招募情况不佳是基于患者“缺陷”模式——无法理解试验过程。沟通不畅也被认为是招募的一个可能障碍。一项定性的患者访谈研究被纳入了一项 III 期非劣效性随机对照试验(SPARE,CRUK/07/011)的可行性阶段,该试验针对肌肉浸润性膀胱癌。目的是阐明随机分组过程中的问题。
定性研究采用“框架分析”,包括“不断比较”,对半结构化访谈进行转录、分析、比较和对比,既在转录之间进行,也在转录内进行。三位研究人员对数据进行编码和解释。
24 名患者同意参加访谈研究;10 名随机分组拒绝者和 14 名接受者,其中 2 名随后拒绝了他们分配的治疗。大多数样本的主要主题是困惑和含糊不清。几乎没有迹象表明困惑直接影响进入 SPARE 试验的决定。然而,困惑似乎确实影响了围绕“知情同意”的伦理考虑,以及在患者和卫生人员之间造成一种疏远感。许多方面的沟通不佳导致了困惑,加上试验的后勤元素,涉及在多个地理位置提供治疗选择。
这些数据突出表明,尽管有最好的意图,但在英国卫生系统中提供平衡和清晰的试验信息具有一定难度。多名专业人员的参与可能会影响考虑参与 RCT 的患者的沟通过程。我们的结果使我们对患者行为的“缺陷”模式提出了质疑。建议卫生专业人员考虑促进一种环境,使患者感到完全参与试验事业,并可能考虑在测试复杂干预措施时替代随机分组。
ISRCTN61126465。