Department of Nephrology, University Medical Center Groningen, Groningen, The Netherlands.
Diabetes Care. 2013 Jul;36(7):1926-32. doi: 10.2337/dc12-1894. Epub 2013 Feb 1.
Chronic exposure to calcineurin inhibitors and corticosteroids poses renal transplant recipients (RTR) at high risk for development of new-onset diabetes after transplantation (NODAT). Pancreatic β-cell dysfunction may be crucial to the pathophysiology of NODAT and specific markers for β-cell dysfunction may have additive value for predicting NODAT in this population. Therefore, we prospectively investigated whether proinsulin, as a marker of pancreatic β-cell dysfunction, is associated with future development of NODAT and improves prediction of it.
All RTR between 2001 and 2003 with a functioning graft for ≥1 year were considered eligible for inclusion, except for subjects with diabetes at baseline who were excluded. We recorded incidence of NODAT until April 2012.
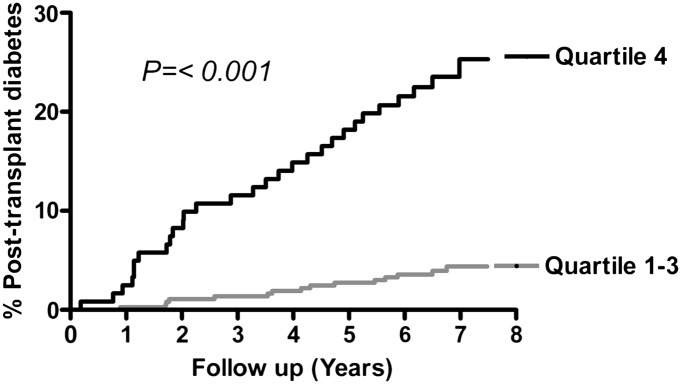
A total of 487 RTR (age 50 ± 12 years, 55% men) participated at a median time of 6.0 (interquartile range [IQR], 2.6-11.5) years after transplantation. Median fasting proinsulin levels were 16.6 (IQR, 11.0-24.2) pmol/L. During median follow-up for 10.1 (IQR, 9.1-10.4) years, 42 (35%) RTR had development of NODAT in the highest quartile of the distribution of proinsulin versus 34 (9%) in the lowest three quartiles (P < 0.001). In Cox regression analyses, proinsulin (hazard ratio, 2.29; 95% CI, 1.85-2.83; P < 0.001) was strongly associated with NODAT development. This was independent of age, sex, calcineurine inhibitors, prednisolone use, components of the metabolic syndrome, or homeostasis model assessment.
In conclusion, fasting proinsulin is strongly associated with NODAT development in RTR. Our results highlight the role of β-cell dysfunction in the pathophysiology of NODAT and indicate the potential value of proinsulin for identification of RTR at increased risk for NODAT.
钙调磷酸酶抑制剂和皮质类固醇的慢性暴露使肾移植受者(RTR)发生移植后新发糖尿病(NODAT)的风险很高。β 细胞功能障碍可能是 NODAT 病理生理学的关键,β 细胞功能障碍的特定标志物可能对预测该人群中的 NODAT 具有附加价值。因此,我们前瞻性地研究了作为β细胞功能障碍标志物的胰岛素原是否与 NODAT 的未来发展相关,以及是否可以改善对其的预测。
所有 2001 年至 2003 年间接受移植且移植后至少 1 年功能正常的 RTR 均符合入选条件,除外基线时患有糖尿病的患者。我们记录了截止到 2012 年 4 月 NODAT 的发病情况。
共有 487 名 RTR(年龄 50 ± 12 岁,55%为男性)参与了研究,移植后中位时间为 6.0(四分位距 [IQR],2.6-11.5)年。空腹胰岛素原中位水平为 16.6(IQR,11.0-24.2)pmol/L。在中位随访 10.1(IQR,9.1-10.4)年期间,胰岛素原分布最高四分位数的 42(35%)名 RTR 发生了 NODAT,而分布最低三分位的 34(9%)名 RTR 发生了 NODAT(P < 0.001)。在 Cox 回归分析中,胰岛素原(风险比,2.29;95%CI,1.85-2.83;P < 0.001)与 NODAT 发展密切相关。这与年龄、性别、钙调磷酸酶抑制剂、泼尼松龙的使用、代谢综合征的组成部分或稳态模型评估无关。
总之,空腹胰岛素原与 RTR 中 NODAT 的发展密切相关。我们的结果强调了β细胞功能障碍在 NODAT 病理生理学中的作用,并表明胰岛素原在识别发生 NODAT 风险增加的 RTR 方面具有潜在价值。