Baade Peter D, Youlden Danny R, Andersson Therese M-L, Youl Philippa H, Kimlin Michael G, Aitken Joanne F, Biggar Robert J
Cancer Council Queensland, Brisbane, Queensland, Australia School of Public Health and Social Work, Queensland University of Technology, Brisbane, Queensland, Australia Menzies Health Institute Queensland, Griffith University, Gold Coast, Queensland, Australia.
Cancer Council Queensland, Brisbane, Queensland, Australia.
BMJ Open. 2015 Apr 13;5(4):e006740. doi: 10.1136/bmjopen-2014-006740.
Communication of relevant prognostic information is critical in helping patients understand the implications of their cancer diagnosis. We describe measures of prognosis to help communicate relevant prognostic information to improve patients' understanding of the implications of their cancer diagnosis.
Australia-wide population-based cancer registry cohort.
870,878 patients aged 15-89 years diagnosed with invasive cancer between 1990 and 2007, with mortality follow-up information to December 2010.
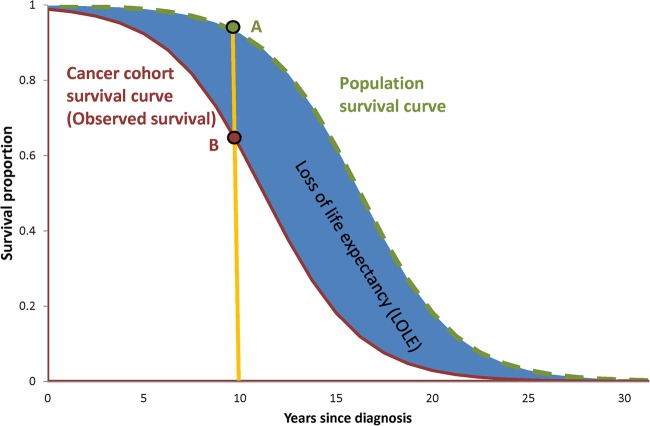
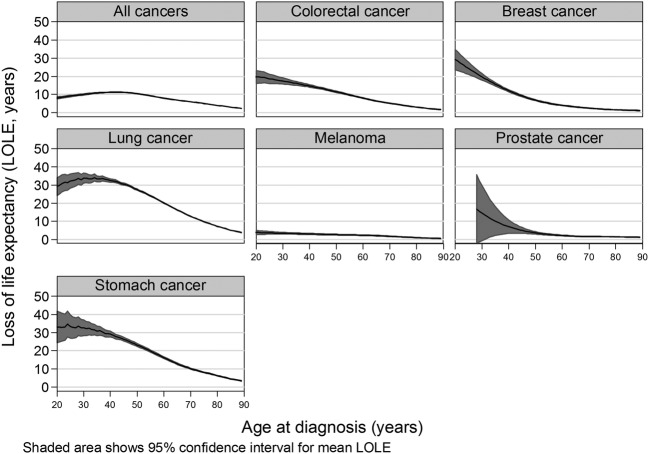
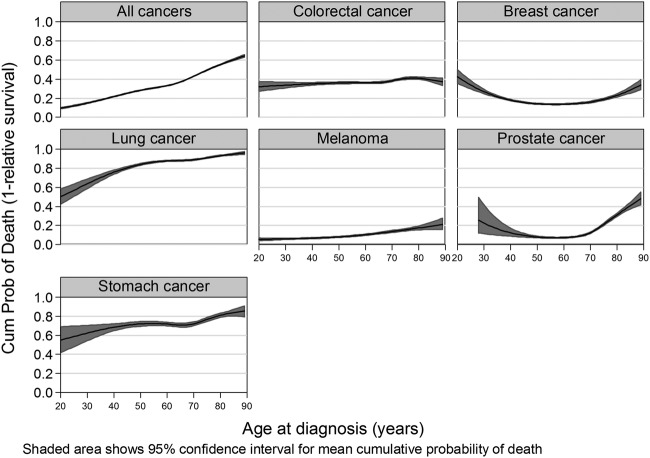
Flexible parametric models were used to estimate loss of life expectancy (LOLE), remaining life expectancy (RLE) and 10-year cumulative probability of cancer-specific death (1-relative survival).
On average, Australians diagnosed with cancer at age 40 years faced losing an average of 11.2 years of life (95% CI 11.1 to 11.4) due to their cancer, while those diagnosed at 80 years faced losing less, an average of 3.9 years (3.9 to 4.0) because of higher competing mortality risks. In contrast, younger people had lower estimated cumulative probabilities of cancer-specific death within 10 years (40 years: 21.5%, 21.4% to 22.1%) compared with older people (80 years: 55.4%, 55.0% to 55.9%). The patterns for individual cancers varied widely, both by cancer type and by age within cancer type.
The LOLE and RLE measures provide complementary messages to standard relative survival estimates (expressed here in terms of cumulative probability of cancer-specific death). Importantly, relative survival per se underplays the greater absolute impact that a cancer diagnosis has at a younger age on LOLE. When presented in isolation for all cancers, it may provide a misleading impression of future mortality burden of cancer overall, and furthermore, it will obscure patterns of mortality by type and by age data within type. Alternative measures of LOLE, therefore, provide important communication about mortality risk to patients with cancer worldwide and should be incorporated into standard reporting and dissemination strategies.
传达相关预后信息对于帮助患者理解其癌症诊断的影响至关重要。我们描述了预后指标,以帮助传达相关预后信息,从而提高患者对其癌症诊断影响的理解。
基于澳大利亚全国人口的癌症登记队列。
1990年至2007年间诊断为浸润性癌症的870878名年龄在15 - 89岁的患者,随访至2010年12月的死亡率信息。
使用灵活的参数模型来估计预期寿命损失(LOLE)、剩余预期寿命(RLE)和癌症特异性死亡的10年累积概率(1 - 相对生存率)。
平均而言,40岁被诊断患有癌症的澳大利亚人由于癌症平均面临损失11.2年的生命(95%可信区间11.1至11.4),而80岁被诊断的人由于更高的竞争死亡风险面临的损失较少,平均为3.9年(3.9至4.0)。相比之下,年轻人在10年内癌症特异性死亡的估计累积概率较低(40岁:21.5%,21.4%至22.1%),而老年人(80岁:55.4%,55.0%至55.9%)。个体癌症的模式差异很大,既因癌症类型而异,也因癌症类型内的年龄而异。
预期寿命损失(LOLE)和剩余预期寿命(RLE)指标为标准相对生存估计(在此以癌症特异性死亡的累积概率表示)提供了补充信息。重要的是,相对生存本身低估了癌症诊断在年轻时对预期寿命损失(LOLE)的更大绝对影响。当单独呈现所有癌症的数据时,它可能会对癌症总体未来的死亡负担产生误导性印象,此外,它会掩盖按类型以及按类型内年龄数据的死亡模式。因此,预期寿命损失(LOLE)的替代指标为全球癌症患者提供了关于死亡风险的重要信息,应纳入标准报告和传播策略中。