Cassol Edana, Rossouw Theresa, Malfeld Susan, Mahasha Phetole, Slavik Tomas, Seebregts Chris, Bond Robert, du Plessis Johannie, Janssen Carl, Roskams Tania, Nevens Frederik, Alfano Massimo, Poli Guido, van der Merwe Schalk W
MRC Unit for Inflammation and Immunity, Department of Immunology and the Tshwane Academic Division of the National Health Laboratory Service, University of Pretoria, Pretoria, South Africa.
Department of Health Sciences, Carleton University, 5433 Herzberg Laboratories, 1125 Colonel By Drive, Ottawa, Ontario, K1S 5B6, Canada.
BMC Infect Dis. 2015 Oct 17;15:430. doi: 10.1186/s12879-015-1176-5.
Intestinal macrophages are key regulators of inflammatory responses to the gut microbiome and play a central role in maintaining tissue homeostasis and epithelial integrity. However, little is known about the role of these cells in HIV infection, a disease fuelled by intestinal inflammation, a loss of epithelial barrier function and increased microbial translocation (MT).
Phenotypic and functional characterization of intestinal macrophages was performed for 23 African AIDS patients with chronic diarrhea and/or weight loss and 11 HIV-negative Africans with and without inflammatory bowel disease (IBD). AIDS patients were treated with cotrimoxazole for the prevention of opportunistic infections (OIs). Macrophage phenotype was assessed by flow cytometry and immuno-histochemistry (IHC); production of proinflammatory mediators by IHC and Qiagen PCR Arrays; in vitro secretion of cytokines by the Bio-Plex Suspension Array System. Statistical analyses were performed using Spearman's correlation and Wilcoxon matched-pair tests. Results between groups were analyzed using the Kruskal-Wallis with Dunn's post-test and the Mann-Whitney U tests.
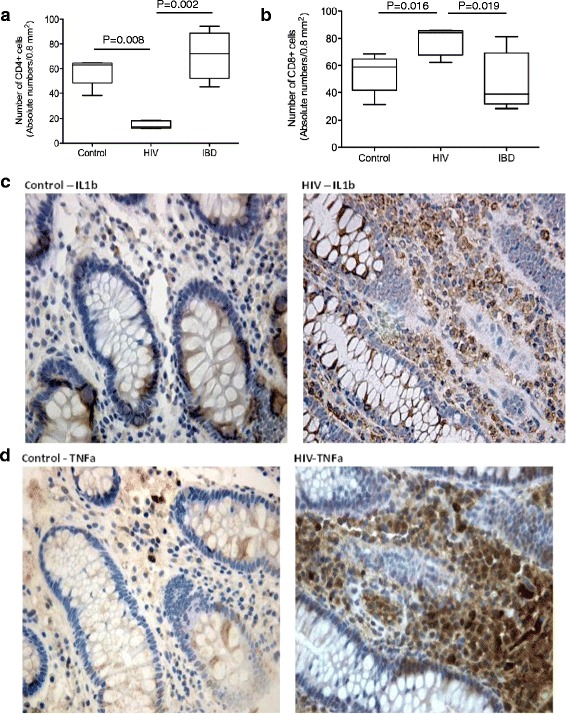
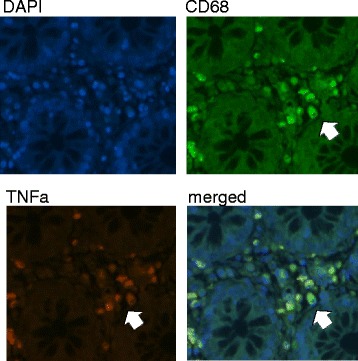
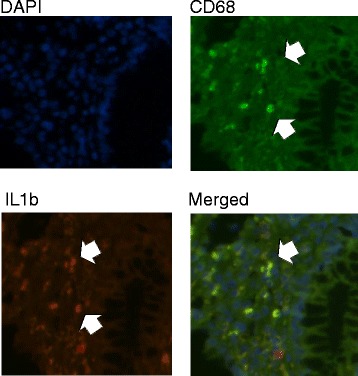
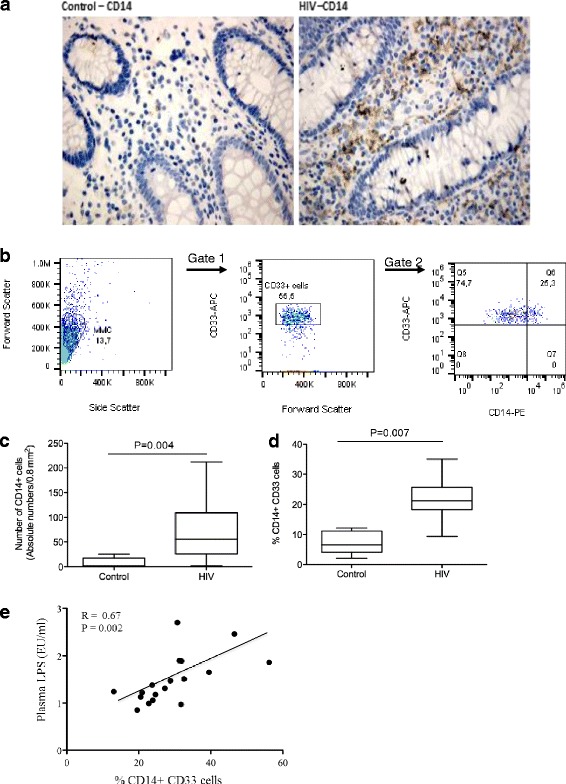
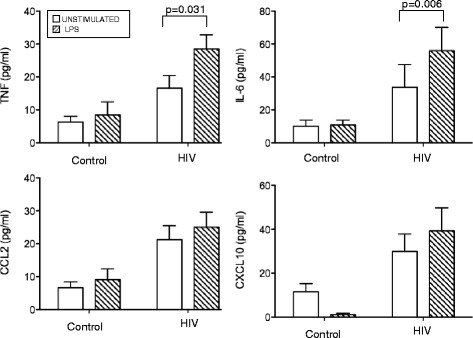
None of the study participants had evidence of enteric co-infections as assessed by stool analysis and histology. Compared to healthy HIV-negative controls, the colon of AIDS patients was highly inflamed with increased infiltration of inflammatory cells and increased mRNA expression of proinflammatory cytokine (tumour necrosis factor (TNF)-α, interleukin (IL)-1β, IFN-γ, and IL-18), chemokines (chemokine (C-C motif) ligand (CCL)2 and chemokine (C-X-C) motif ligand (CXCL)10) and transcription factors (TNF receptor-associated factor (TRAF)6 and T-box (TXB)21). IHC revealed significant co-localization of TNF-α and IL-1β with CD68(+) cells. As in IBD, HIV was associated with a marked increase in macrophages expressing innate response receptors including CD14, the co-receptor for lipopolysaccharide (LPS). The frequency of CD14(+) macrophages correlated positively with plasma LPS, a marker of MT. Total unfractionated mucosal mononuclear cells (MMC) isolated from the colon of AIDS patients, but not MMC depleted of CD14(+) cells, secreted increased levels of proinflammatory cytokines ex vivo in response to LPS.
Intestinal macrophages, in the absence of overt OIs, play an important role in driving persistent inflammation in HIV patients with late-stage disease and diarrhea. These results suggest intensified treatment strategies that target inflammatory processes in intestinal macrophages may be highly beneficial in restoring the epithelial barrier and limiting MT in HIV-infected patients.
肠道巨噬细胞是对肠道微生物群炎症反应的关键调节因子,在维持组织稳态和上皮完整性方面发挥核心作用。然而,对于这些细胞在HIV感染中的作用知之甚少,HIV感染是一种由肠道炎症、上皮屏障功能丧失和微生物易位(MT)增加所引发的疾病。
对23例患有慢性腹泻和/或体重减轻的非洲艾滋病患者以及11例有或无炎症性肠病(IBD)的HIV阴性非洲人进行肠道巨噬细胞的表型和功能特征分析。艾滋病患者接受复方新诺明治疗以预防机会性感染(OIs)。通过流式细胞术和免疫组织化学(IHC)评估巨噬细胞表型;通过IHC和Qiagen PCR阵列检测促炎介质的产生;利用Bio-Plex悬浮阵列系统检测细胞因子的体外分泌。使用Spearman相关性分析和Wilcoxon配对检验进行统计分析。组间结果采用Kruskal-Wallis检验及Dunn事后检验和Mann-Whitney U检验进行分析。
通过粪便分析和组织学评估,所有研究参与者均无肠道合并感染的证据。与健康的HIV阴性对照相比,艾滋病患者的结肠高度发炎,炎症细胞浸润增加,促炎细胞因子(肿瘤坏死因子(TNF)-α、白细胞介素(IL)-1β、干扰素-γ和IL-18)、趋化因子(趋化因子(C-C基序)配体(CCL)2和趋化因子(C-X-C)基序配体(CXCL)10)以及转录因子(TNF受体相关因子(TRAF)6和T盒(TXB)21)的mRNA表达增加。IHC显示TNF-α和IL-1β与CD68(+)细胞有显著共定位。与IBD一样,HIV与表达包括CD14(脂多糖(LPS)的共受体)在内的先天反应受体的巨噬细胞显著增加有关。CD14(+)巨噬细胞的频率与MT标志物血浆LPS呈正相关。从艾滋病患者结肠分离的未分级黏膜单核细胞(MMC),而非耗尽CD14(+)细胞的MMC,在体外对LPS刺激反应时分泌的促炎细胞因子水平增加。
在没有明显机会性感染的情况下,肠道巨噬细胞在驱动晚期疾病和腹泻的HIV患者持续炎症中起重要作用。这些结果表明,针对肠道巨噬细胞炎症过程的强化治疗策略可能对恢复上皮屏障和限制HIV感染患者的MT非常有益。