Furuya-Kanamori Luis, Liang Shaohong, Milinovich Gabriel, Soares Magalhaes Ricardo J, Clements Archie C A, Hu Wenbiao, Brasil Patricia, Frentiu Francesca D, Dunning Rebecca, Yakob Laith
Research School of Population Health, Australian National University, Acton, ACT 2601, Australia.
Environmental Health Institute, National Environment Agency, Singapore, 138667, Singapore.
BMC Infect Dis. 2016 Mar 3;16:84. doi: 10.1186/s12879-016-1417-2.
Chikungunya and dengue infections are spatio-temporally related. The current review aims to determine the geographic limits of chikungunya, dengue and the principal mosquito vectors for both viruses and to synthesise current epidemiological understanding of their co-distribution.
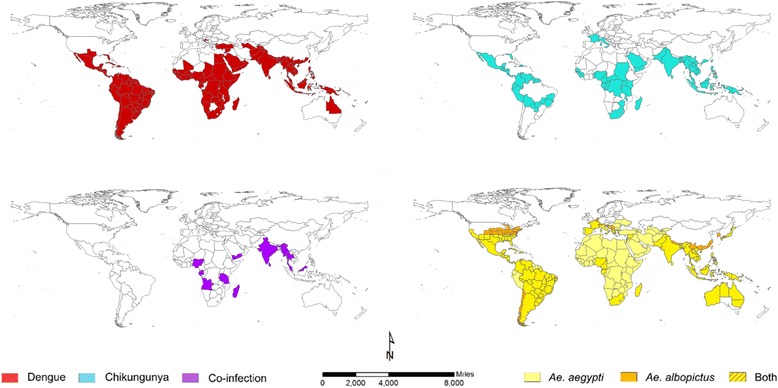
Three biomedical databases (PubMed, Scopus and Web of Science) were searched from their inception until May 2015 for studies that reported concurrent detection of chikungunya and dengue viruses in the same patient. Additionally, data from WHO, CDC and Healthmap alerts were extracted to create up-to-date global distribution maps for both dengue and chikungunya.
Evidence for chikungunya-dengue co-infection has been found in Angola, Gabon, India, Madagascar, Malaysia, Myanmar, Nigeria, Saint Martin, Singapore, Sri Lanka, Tanzania, Thailand and Yemen; these constitute only 13 out of the 98 countries/territories where both chikungunya and dengue epidemic/endemic transmission have been reported.
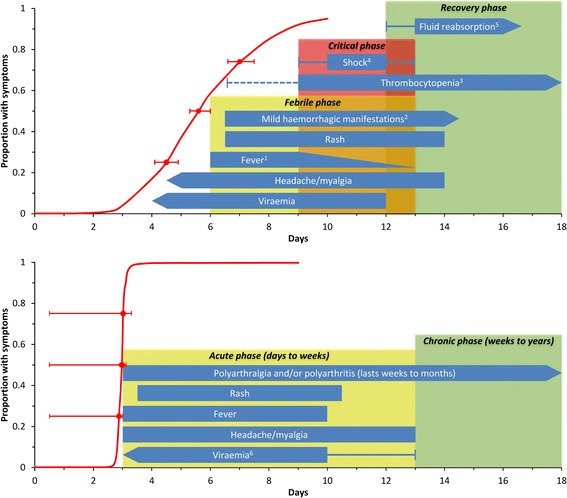
Understanding the true extent of chikungunya-dengue co-infection is hampered by current diagnosis largely based on their similar symptoms. Heightened awareness of chikungunya among the public and public health practitioners in the advent of the ongoing outbreak in the Americas can be expected to improve diagnostic rigour. Maps generated from the newly compiled lists of the geographic distribution of both pathogens and vectors represent the current geographical limits of chikungunya and dengue, as well as the countries/territories at risk of future incursion by both viruses. These describe regions of co-endemicity in which lab-based diagnosis of suspected cases is of higher priority.
基孔肯雅热和登革热感染在时空上存在关联。本综述旨在确定基孔肯雅热、登革热的地理分布范围以及这两种病毒的主要蚊媒,并综合当前对它们共同分布的流行病学认识。
检索了三个生物医学数据库(PubMed、Scopus和Web of Science)自建库起至2015年5月期间报告在同一患者中同时检测到基孔肯雅病毒和登革热病毒的研究。此外,提取了世界卫生组织、美国疾病控制与预防中心以及健康地图警报的数据,以绘制登革热和基孔肯雅热最新的全球分布图。
在安哥拉、加蓬、印度、马达加斯加、马来西亚、缅甸、尼日利亚、圣马丁、新加坡、斯里兰卡、坦桑尼亚、泰国和也门发现了基孔肯雅热 - 登革热合并感染的证据;在报告有基孔肯雅热和登革热流行/地方性传播的98个国家/地区中,这些国家仅占13个。
目前主要基于相似症状进行诊断,这妨碍了对基孔肯雅热 - 登革热合并感染真实情况的了解。在美洲当前疫情爆发的情况下,提高公众和公共卫生从业者对基孔肯雅热的认识,有望提高诊断的严谨性。根据新编制的病原体和病媒地理分布清单生成的地图,代表了基孔肯雅热和登革热目前的地理分布范围,以及这两种病毒未来可能入侵的国家/地区。这些地图描述了共地方病流行区域,在这些区域对疑似病例进行实验室诊断具有更高的优先级。