aDepartment of Anesthesiology and Pediatrics (Nutrition Section), University of Colorado Denver, Denver, Colorado bInstitute for Systems Biology, Seattle, Washington cDepartment of Pediatrics, University of California, San Diego, San Diego, California, USA.
Curr Opin Crit Care. 2016 Aug;22(4):347-53. doi: 10.1097/MCC.0000000000000321.
Loss of 'health-promoting' microbes and overgrowth of pathogenic bacteria (dysbiosis) in ICU is believed to contribute to nosocomial infections, sepsis, and organ failure (multiple organ dysfunction syndrome). This review discusses new understanding of ICU dysbiosis, new data for probiotics and fecal transplantation in ICU, and new data characterizing the ICU microbiome.
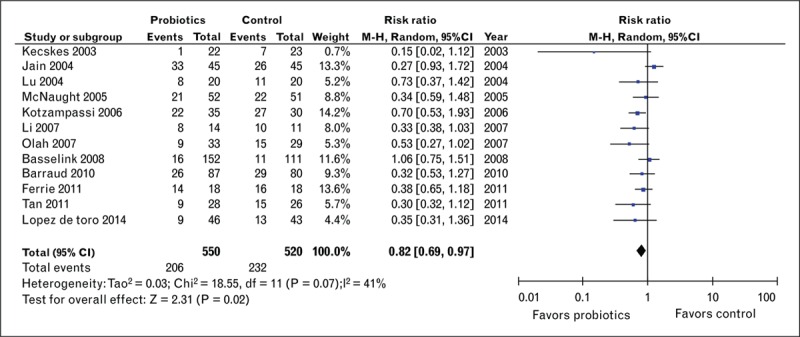
ICU dysbiosis results from many factors, including ubiquitous antibiotic use and overuse. Despite advances in antibiotic therapy, infections and mortality from often multidrug-resistant organisms (i.e., Clostridium difficile) are increasing. This raises the question of whether restoration of a healthy microbiome via probiotics or other 'dysbiosis therapies' would be an optimal alternative, or parallel treatment option, to antibiotics. Recent clinical data demonstrate probiotics can reduce ICU infections and probiotics or fecal microbial transplant (FMT) can treat Clostridium difficile. This contributes to recommendations that probiotics should be considered to prevent infection in ICU. Unfortunately, significant clinical variability limits the strength of current recommendations and further large clinical trials of probiotics and FMT are needed. Before larger trials of 'dysbiosis therapy' can be thoughtfully undertaken, further characterization of ICU dysbiosis is needed. To addressing this, we conducted an initial analysis demonstrating a rapid and marked change from a 'healthy' microbiome to an often pathogen-dominant microbiota (dysbiosis) in a broad ICU population.
A growing body of evidence suggests critical illness and ubiquitous antibiotic use leads to ICU dysbiosis that is associated with increased ICU infection, sepsis, and multiple organ dysfunction syndrome. Probiotics and FMT show promise as ICU therapies for infection. We hope future-targeted therapies using microbiome signatures can be developed to correct 'illness-promoting' dysbiosis to restore a healthy microbiome post-ICU to improve patient outcomes.
目的综述:重症监护病房(ICU)中“促进健康”的微生物丧失和致病菌过度生长(生态失调)被认为会导致医院获得性感染、脓毒症和器官衰竭(多器官功能障碍综合征)。本综述讨论了 ICU 生态失调的新认识、ICU 中益生菌和粪便移植的新数据,以及 ICU 微生物组的新数据。
最新发现:ICU 生态失调是由多种因素引起的,包括广泛使用和过度使用抗生素。尽管抗生素治疗取得了进展,但感染和死亡率不断上升,且经常是多药耐药菌(例如艰难梭菌)所致。这就提出了一个问题,即通过益生菌或其他“生态失调治疗”来恢复健康的微生物组是否是抗生素的最佳替代或平行治疗选择。最近的临床数据表明,益生菌可以减少 ICU 感染,益生菌或粪便微生物移植(FMT)可以治疗艰难梭菌。这有助于建议考虑使用益生菌来预防 ICU 感染。不幸的是,显著的临床变异性限制了现有建议的强度,需要进一步进行益生菌和 FMT 的大型临床试验。在可以慎重地进行更大规模的“生态失调治疗”试验之前,需要进一步对 ICU 生态失调进行特征描述。为了解决这个问题,我们进行了一项初步分析,结果表明,在广泛的 ICU 人群中,从“健康”微生物组到通常以病原体为主的微生物组(生态失调)的快速而显著的变化。
总结:越来越多的证据表明,严重疾病和广泛使用抗生素会导致 ICU 生态失调,从而增加 ICU 感染、脓毒症和多器官功能障碍综合征的风险。益生菌和 FMT 作为 ICU 感染的治疗方法有一定的前景。我们希望能够开发出针对未来的靶向治疗方法,利用微生物组特征来纠正“促进疾病”的生态失调,恢复 ICU 后健康的微生物组,以改善患者的预后。