Aghajafari Fariba, Field Catherine J, Kaplan Bonnie J, Rabi Doreen M, Maggiore Jack A, O'Beirne Maeve, Hanley David A, Eliasziw Misha, Dewey Deborah, Weinberg Amy, Ross Sue J
Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Department of Agricultural, Food and Nutritional Science, University of Alberta, Edmonton, Alberta, Canada.
PLoS One. 2016 Jul 1;11(7):e0157262. doi: 10.1371/journal.pone.0157262. eCollection 2016.
The aims of this study were to determine if pregnant women consumed the recommended vitamin D through diet alone or through diet and supplements, and if they achieved the current reference range vitamin D status when their reported dietary intake met the current recommendations.
Data and banked blood samples collected in second trimester from a subset of 537 women in the APrON (Alberta Pregnant Outcomes and Nutrition) study cohort were examined. Frozen collected plasma were assayed using LC-MS/MS (liquid chromatography-tandem mass spectrometry) to determine 25(OH)D2, 25(OH)D3, 3-epi-25(OH)D3 concentrations. Dietary data were obtained from questionnaires including a Supplement Intake Questionnaire and a 24-hour recall of the previous day's diet.
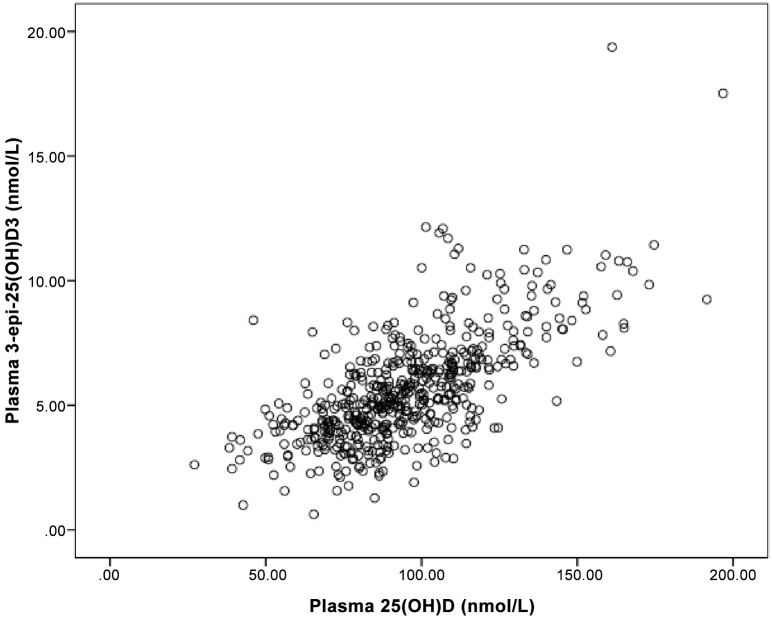
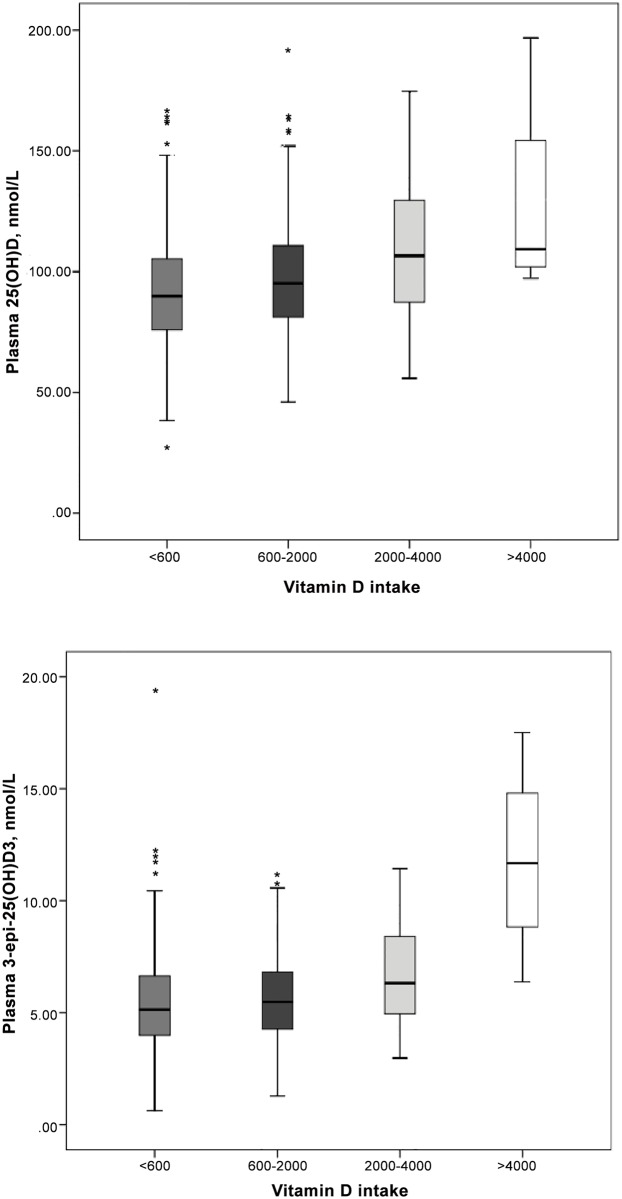
Participants were 87% Caucasian; mean (SD) age of 31.3 (4.3); BMI 25.8 (4.7); 58% were primiparous; 90% had education beyond high school; 80% had a family income higher than CAN $70,000/year. 25(OH)D2, 25(OH)D3, and 3-epi-25(OH)D3) were identified in all of the 537 plasma samples;3-epi-25(OH)D3 contributed 5% of the total vitamin D. The median (IQR) total 25(OH)D (D2+D3) was 92.7 (30.4) nmol/L and 20% of women had 25(OH)D concentration < 75 nmol/L. The median (IQR) reported vitamin D intake from diet and supplements was 600 (472) IU/day. There was a significant relationship between maternal reported dietary vitamin D intake (diet and supplement) and 25(OH)D and 3-epi-25(OH)D3 concentrations in an adjusted linear regression model.
We demonstrated the current RDA (600 IU/ day) may not be adequate to achieve vitamin D status >75 nmol/L in some pregnant women who are residing in higher latitudes (Calgary, 51°N) in Alberta, Canada and the current vitamin D recommendations for Canadian pregnant women need to be re-evaluated.
本研究的目的是确定孕妇是否仅通过饮食或通过饮食与补充剂摄入了推荐量的维生素D,以及当她们报告的饮食摄入量符合当前建议时,其维生素D状态是否达到了当前参考范围。
对阿尔伯塔省孕期结局与营养(APrON)研究队列中537名妇女的一个子集在孕中期收集的数据和储存的血样进行了检查。使用液相色谱-串联质谱法(LC-MS/MS)对冷冻收集的血浆进行检测,以测定25(OH)D2、25(OH)D3、3-表-25(OH)D3的浓度。饮食数据来自问卷调查,包括补充剂摄入问卷和前一天饮食的24小时回顾。
参与者中87%为白种人;平均(标准差)年龄31.3(4.3)岁;体重指数25.8(4.7);58%为初产妇;90%接受过高中以上教育;80%家庭收入高于每年7万加元。在所有537份血浆样本中均检测到25(OH)D2、25(OH)D3和3-表-25(OH)D3;3-表-25(OH)D3占总维生素D的5%。25(OH)D(D2+D3)的中位数(四分位间距)为92.7(30.4)nmol/L,20%的妇女25(OH)D浓度<75 nmol/L。饮食和补充剂中维生素D摄入量的中位数(四分位间距)为600(472)IU/天。在调整后的线性回归模型中,母亲报告的饮食中维生素D摄入量(饮食和补充剂)与25(OH)D和3-表-25(OH)D3浓度之间存在显著关系。
我们证明,对于居住在加拿大阿尔伯塔省较高纬度地区(卡尔加里,北纬51°)的一些孕妇,目前的膳食参考摄入量(600 IU/天)可能不足以使维生素D水平>75 nmol/L,加拿大目前对孕妇的维生素D建议需要重新评估。