Verberne Steven J, Sonnega Remko J A, Temmerman Olivier P P, Raijmakers Pieter G
Department of Orthopaedics, Noordwest Ziekenhuisgroep, Wilhelminalaan 12, 1815 JD, Alkmaar, NWZ, The Netherlands.
The Centre for Orthopaedic Research Alkmaar (CORAL), Noordwest Ziekenhuisgroep, Alkmaar, The Netherlands.
Clin Orthop Relat Res. 2017 May;475(5):1395-1410. doi: 10.1007/s11999-016-5218-0. Epub 2017 Jan 3.
In the assessment of possible periprosthetic knee infection, various imaging modalities are used without consensus regarding the most accurate technique.
QUESTIONS/PURPOSES: To perform a meta-analysis to compare the accuracy of various applied imaging modalities in the assessment of periprosthetic knee infection.
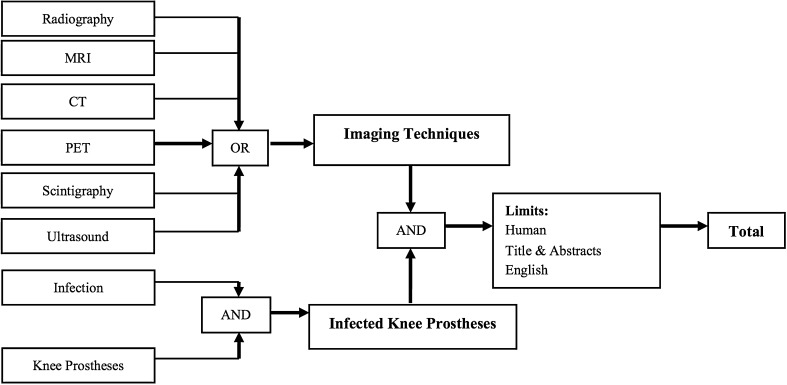
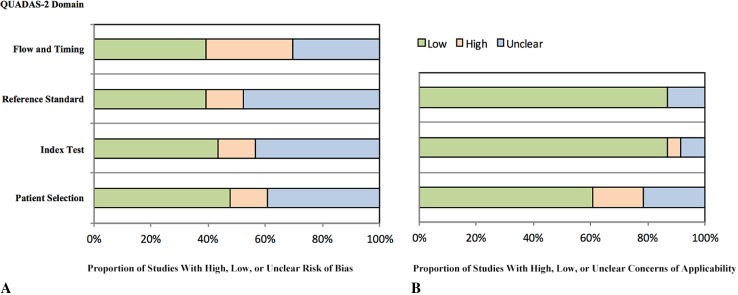
A systematic review and meta-analysis was conducted with a comprehensive search of MEDLINE and Embase in accordance with the PRISMA and Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) recommendations to identify clinical studies in which periprosthetic knee infection was investigated with different imaging modalities. The sensitivity and specificity of each imaging technique were determined and compared with the results of microbiologic and histologic analyses, intraoperative findings, and clinical followup of more than 6 months. A total of 23 studies, published between 1990 and 2015, were included for meta-analysis, representing 1027 diagnostic images of symptomatic knee prostheses. Quality of the included studies showed low concerns regarding external validity, whereas internal validity indicated more concerns regarding the risk of bias. The most important concerns were found in the lack of uniform criteria for the diagnosis of a periprosthetic infection and the flow and timing of the included studies. Differences among techniques were tested at a probability less than 0.05 level. Where there was slight overlap of confidence intervals for two means, it is possible for the point estimates to be statistically different from one another at a probability less than 0.05. The z-test was used to statistically analyze differences in these situations.
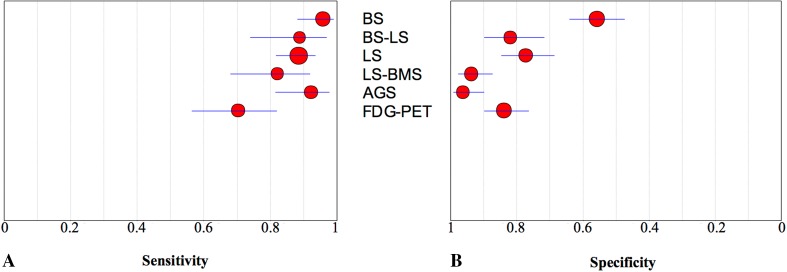
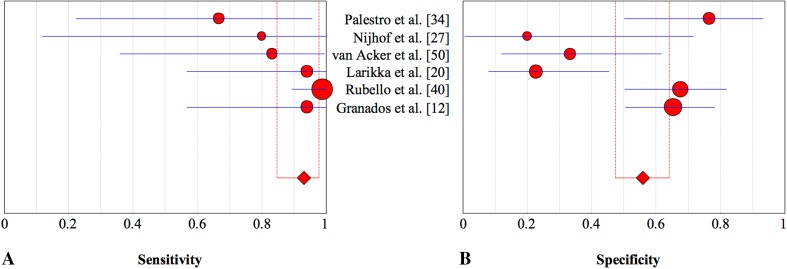
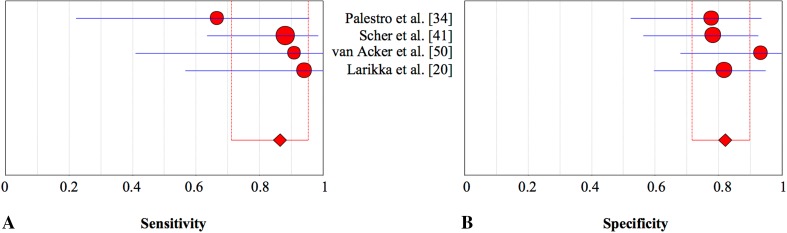
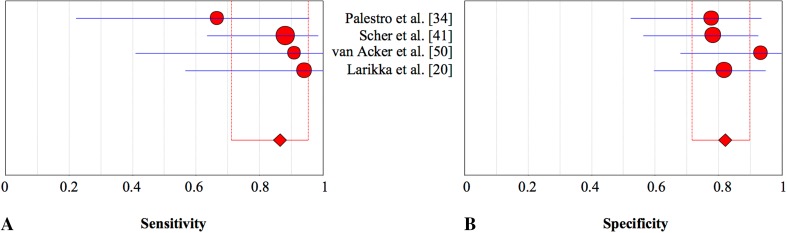
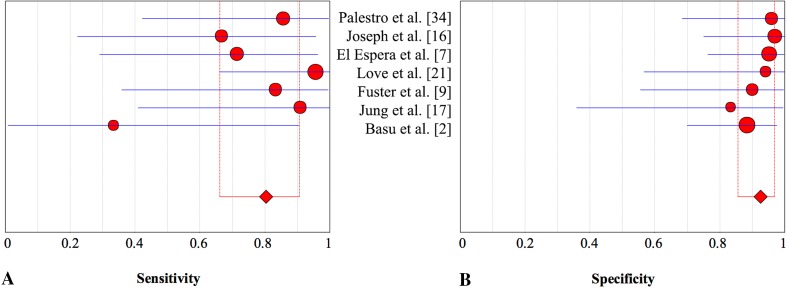
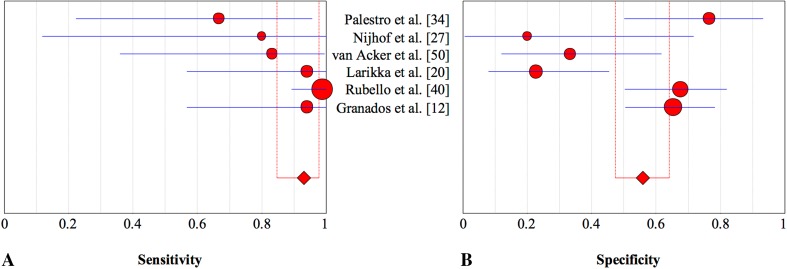
Bone scintigraphy was less specific than all other modalities tested (56%; 95% CI, 0.47-0.64; p < 0.001), and leukocyte scintigraphy (77%; 95% CI, 0.69-0.85) was less specific than antigranulocyte scintigraphy (95%; 95% CI, 0.88-0.98; p < 0.001) or combined leukocyte and bone marrow scintigraphy (93%; 95% CI, 0.86-0.97; p < 0.001). Fluorodeoxyglucose positron emission tomography (FDG-PET) (84%; 95% CI, 0.76-0.90) was more specific than bone scintigraphy (56%; 95% CI, 0.47-0.64; p < 0.001), and less specific than antigranulocyte scintigraphy (95%; 95% CI, 0.88-0.98; p = 0.02) and combined leukocyte and bone marrow scintigraphy (93%; 95% CI, 0.86-0.97; p < 0.001). Leukocyte scintigraphy (88%; 95% CI, 0.81-0.93; p = 0.01) and antigranulocyte scintigraphy (90%; 95% CI, 0.78-0.96; p = 0.02) were more sensitive than FGD-PET (70%; 95% CI, 0.56-0.81). However, because of broad overlapping of confidence intervals, no differences in sensitivity were observed among the other modalities, including combined bone scintigraphy (93%; 95% CI, 0.85-0.98) or combined leukocyte and bone marrow scintigraphy (80%; 95% CI, 0.66-0.91; p > 0.05 for all paired comparisons).
Based on current evidence, antigranulocyte scintigraphy and combined leukocyte and bone marrow scintigraphy appear to be highly specific imaging modalities in confirming periprosthetic knee infection. Bone scintigraphy was a highly sensitive imaging technique but lacks the specificity needed to differentiate among various conditions that cause painful knee prostheses. FDG-PET may not be the preferred imaging modality because it is more expensive and not more effective in confirming periprosthetic knee infection.
Level III, diagnostic study.
在评估可能的人工膝关节周围感染时,会使用多种成像方式,但对于最准确的技术尚无共识。
问题/目的:进行一项荟萃分析,以比较各种应用的成像方式在评估人工膝关节周围感染时的准确性。
按照PRISMA和诊断准确性研究质量评估(QUADAS-2)建议,对MEDLINE和Embase进行全面检索,进行系统评价和荟萃分析,以识别使用不同成像方式研究人工膝关节周围感染的临床研究。确定每种成像技术的敏感性和特异性,并与微生物学和组织学分析结果、术中发现以及超过6个月的临床随访结果进行比较。共有1990年至2015年间发表的23项研究纳入荟萃分析,代表了1027例有症状膝关节假体的诊断图像。纳入研究的质量显示对外在有效性的担忧较低,而内在有效性表明对偏倚风险的担忧更多。发现最重要的问题在于缺乏人工关节周围感染诊断的统一标准以及纳入研究的流程和时间安排。技术之间的差异在概率小于0.05水平进行检验。当两个均值的置信区间存在轻微重叠时,点估计值在概率小于0.05时可能在统计学上彼此不同。在这些情况下使用z检验进行统计学差异分析。
骨闪烁显像的特异性低于所有其他测试方式(56%;95%CI,0.47 - 0.64;p < 0.001),白细胞闪烁显像(77%;95%CI,0.69 - 0.85)的特异性低于抗粒细胞闪烁显像(95%;95%CI,0.88 - 0.98;p < 0.001)或白细胞与骨髓联合闪烁显像(93%;95%CI,0.86 - 0.97;p < 0.001)。氟脱氧葡萄糖正电子发射断层扫描(FDG-PET)(84%;95%CI,0.76 - 0.90)的特异性高于骨闪烁显像(56%;95%CI,0.47 - 0.64;p < 0.001),但低于抗粒细胞闪烁显像(95%;95%CI,0.88 - 0.98;p = 0.02)和白细胞与骨髓联合闪烁显像(93%;95%CI,0.86 - 0.97;p < 0.001)。白细胞闪烁显像(88%;95%CI,0.81 - 0.93;p = 0.01)和抗粒细胞闪烁显像(90%;95%CI,0.78 - 0.96;p = 0.02)比FDG-PET(70%;95%CI,0.56 - 0.81)更敏感。然而,由于置信区间广泛重叠,在包括联合骨闪烁显像(93%;95%CI,0.85 - 0.98)或白细胞与骨髓联合闪烁显像(80%;95%CI,0.66 - 0.91;所有配对比较p > 0.05)在内的其他方式之间未观察到敏感性差异。
基于当前证据,抗粒细胞闪烁显像和白细胞与骨髓联合闪烁显像似乎是确认人工膝关节周围感染的高度特异性成像方式。骨闪烁显像是一种高度敏感成像技术,但缺乏区分导致膝关节假体疼痛的各种情况所需的特异性。FDG-PET可能不是首选成像方式,因为它更昂贵且在确认人工膝关节周围感染方面并不更有效。证据水平:III级,诊断性研究。