Lee Yong Joon, Kim Woo Ram, Han Jeonghee, Han Yoon Dae, Cho Min Soo, Hur Hyuk, Lee Kang Young, Kim Nam Kyu, Min Byung Soh
Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Department of Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
Ann Coloproctol. 2016 Dec;32(6):208-214. doi: 10.3393/ac.2016.32.6.208. Epub 2016 Dec 31.
Previous studies have demonstrated the prognostic impact of the prognostic nutritional index (PNI), a proposed indicator of immunonutritional statuses of surgical patients, on patients with various gastrointestinal cancers. Although the prognostic impact of the PNI on patients with colorectal cancer has been well established, its value has not been studied in patients treated with preoperative chemoradiation (pCRT). This study aimed to evaluate the prognostic impact of PNI on patients receiving pCRT for locally advanced rectal cancer (LARC).
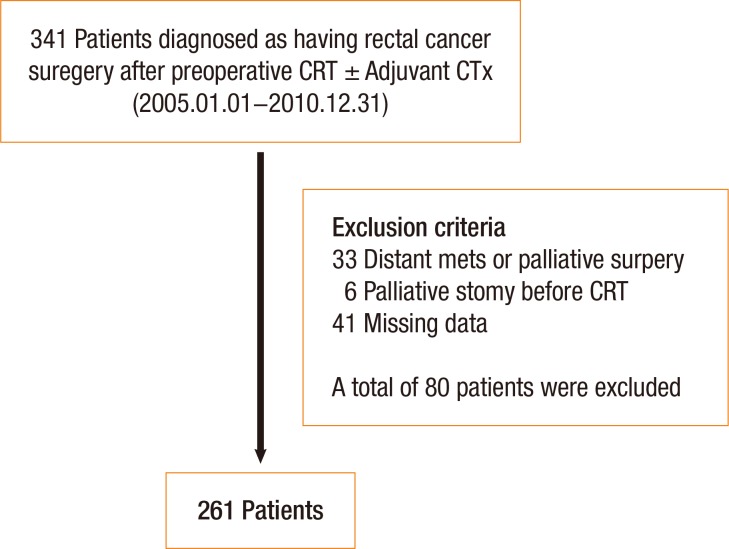
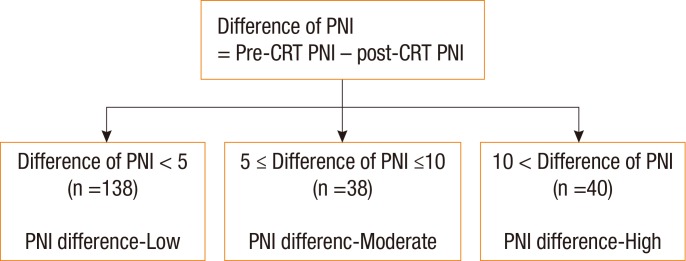
Patients with LARC who underwent curative pCRT followed by surgical resection were enrolled. The PNI was measured in all patients before and after pCRT, and the difference in values was calculated as the PNI difference (dPNI). Patients were classified according to dPNI (<5, 5-10, and >10). Clinicopathologic parameters and long-term oncologic outcomes were assessed according to dPNI classification.
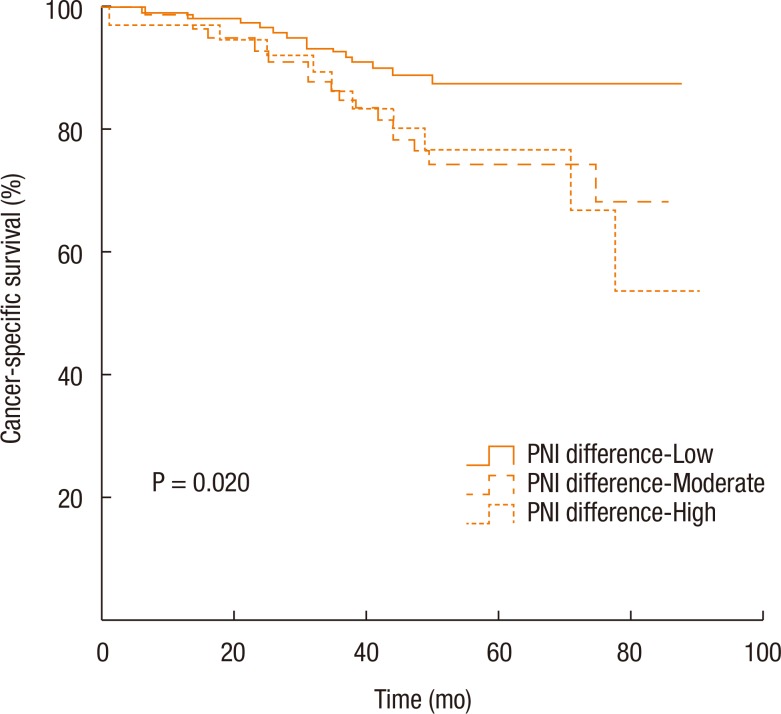
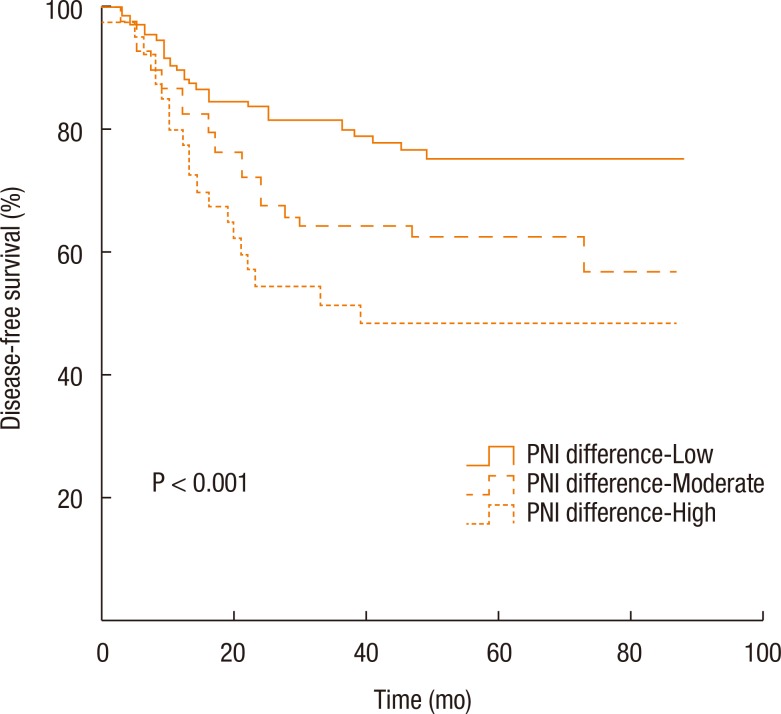
No significant intergroup differences were observed in clinicopathologic parameters such as age, histologic grade, tumor location, tumor-node-metastasis stage, and postoperative complications. Approximately 53% of the patients had a mild dPNI (<5); only 15% had a high dPNI (>10). Univariate and multivariate analyses identified the dPNI as an independent prognostic factor for disease-free status (P < 0.01; hazard ratio [HR], 2.792; 95% confidence interval [CI], 1.577-4.942) and for cancer-specific survival (P = 0.012; HR, 2.469; 95%CI, 1.225-4.978).
The dPNI is predictive of long-term outcomes in pCRT-treated patients with LARC. Further prospective studies should investigate whether immune-nutritional status correction during pCRT would improve oncologic outcomes.
既往研究已证实预后营养指数(PNI)这一外科患者免疫营养状态的拟用指标对各种胃肠道癌症患者的预后影响。尽管PNI对结直肠癌患者的预后影响已得到充分证实,但其在接受术前放化疗(pCRT)的患者中的价值尚未得到研究。本研究旨在评估PNI对局部晚期直肠癌(LARC)接受pCRT患者的预后影响。
纳入接受根治性pCRT后行手术切除的LARC患者。在所有患者pCRT前后测量PNI,并计算其差值作为PNI差值(dPNI)。根据dPNI(<5、5 - 10和>10)对患者进行分类。根据dPNI分类评估临床病理参数和长期肿瘤学结局。
在年龄、组织学分级、肿瘤位置、肿瘤-淋巴结-转移分期和术后并发症等临床病理参数方面,未观察到显著的组间差异。约53%的患者dPNI轻度降低(<5);只有15%的患者dPNI显著降低(>10)。单因素和多因素分析确定dPNI是无病状态(P < 0.01;风险比[HR],2.792;95%置信区间[CI],1.577 - 4.942)和癌症特异性生存(P = 0.012;HR,2.469;95%CI,1.225 - 4.978)的独立预后因素。
dPNI可预测pCRT治疗的LARC患者的长期结局。进一步的前瞻性研究应调查在pCRT期间纠正免疫营养状态是否会改善肿瘤学结局。