Gottlieb Klaus, Le Chenxiong, Wacher Vince, Sliman Joe, Cruz Christine, Porter Tyler, Carter Stephen
Synthetic Biologics Inc., Rockville, Maryland, USA
Synthetic Biologics Inc., Rockville, Maryland, USA.
Gastroenterol Rep (Oxf). 2017 Aug;5(3):193-199. doi: 10.1093/gastro/gow048. Epub 2017 Jan 27.
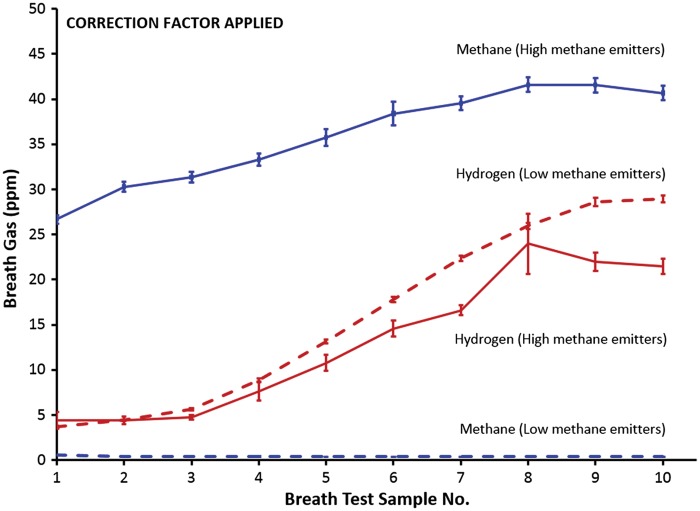
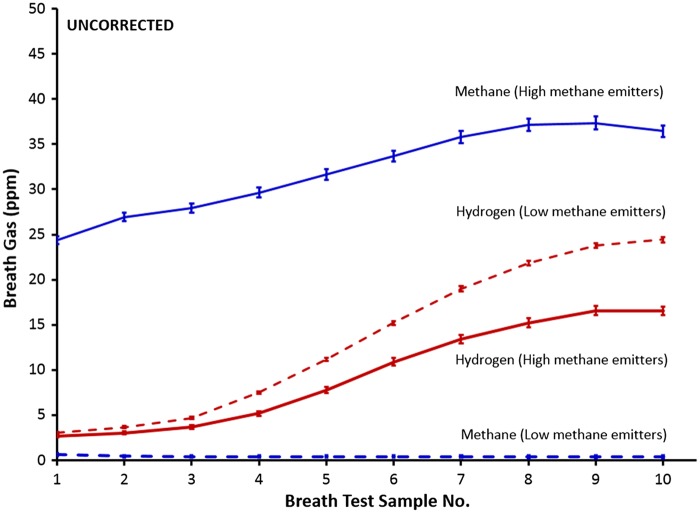
Levels of breath methane, together with breath hydrogen, are determined by means of repeated collections of both, following ingestion of a carbohydrate substrate, at 15-20 minutes intervals, until 10 samples have been obtained. The frequent sampling is required to capture a rise of hydrogen emissions, which typically occur later in the test: in contrast, methane levels are typically elevated at baseline. If methane emissions represent the principal objective of the test, a spot methane test (i.e. a single-time-point sample taken after an overnight fast without administration of substrate) may be sufficient.
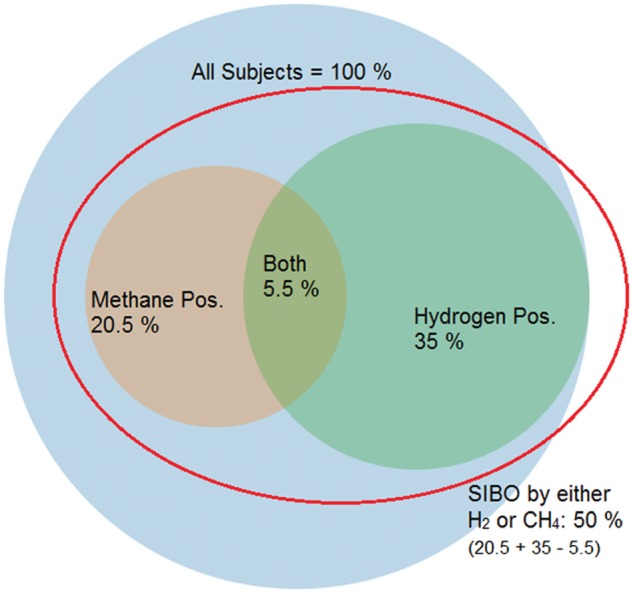
We analysed 10-sample lactulose breath test data from 11 674 consecutive unique subjects who submitted samples to Commonwealth Laboratories (Salem, MA, USA) from sites in all of the states of the USA over a one-year period. The North American Consensus (NAC) guidelines criteria for breath testing served as a reference standard.
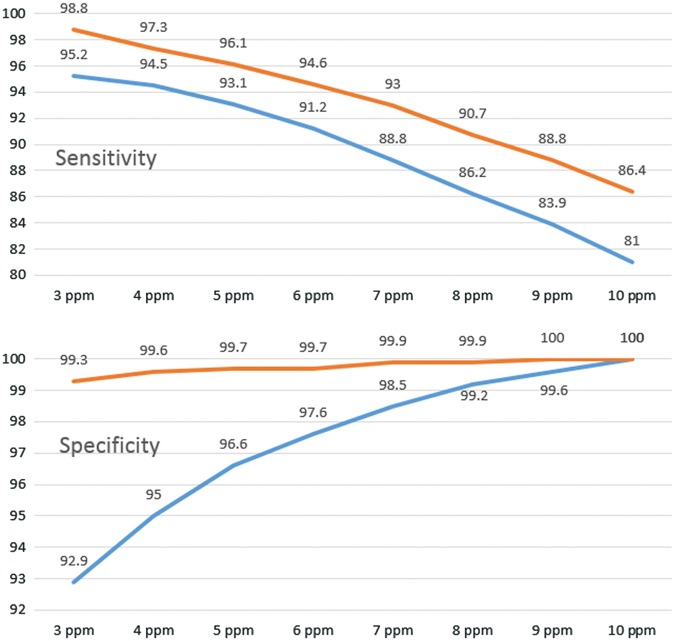
The overall prevalence of methane-positive subjects (by NAC criteria) was 20.4%, based on corrected methane results, and 18.9% based on raw data. In our USA dataset, the optimal cut-off level to maximize sensitivity and specificity was ≥4 ppm CH, 94.5% [confidential interval (CI): 93.5-95.4%] and 95.0% (CI: 94.6-95.5%), respectively. The use of a correction factor (CF) (5% CO as numerator) led to reclassifications CH-high to CH-low in 0.7 % and CH-low to CH-high in 2.1%.
A cut-off value for methane at baseline of either ≥4 ppm, as in our USA dataset, or ≥ 5 ppm, as described in a single institution study, are both highly accurate in identifying subjects at baseline that would be diagnosed as 'methane-positive' in a 10-sample lactulose breath test for small intestinal bacterial overgrowth.
呼气甲烷水平与呼气氢气水平通过在摄入碳水化合物底物后,每隔15 - 20分钟重复收集两者来测定,直至获得10份样本。需要频繁采样以捕捉氢气排放的上升,这通常在测试后期出现;相比之下,甲烷水平在基线时通常就会升高。如果甲烷排放是测试的主要目标,单次甲烷测试(即在禁食过夜且未给予底物后采集的单点样本)可能就足够了。
我们分析了来自11674名连续且唯一的受试者的10份样本乳果糖呼气测试数据,这些受试者在一年时间内从美国所有州的地点向英联邦实验室(美国马萨诸塞州塞勒姆)提交了样本。北美共识(NAC)呼气测试指南标准作为参考标准。
根据校正后的甲烷结果,甲烷阳性受试者的总体患病率(按照NAC标准)为20.4%,基于原始数据为18.9%。在我们的美国数据集中,使敏感性和特异性最大化的最佳截断水平为≥4 ppm CH,敏感性为94.5% [置信区间(CI):93.5 - 95.4%],特异性为95.0%(CI:94.6 - 95.5%)。使用校正因子(CF)(以5% CO作为分子)导致0.7%的CH高被重新分类为CH低,2.1%的CH低被重新分类为CH高。
在美国数据集中,基线时甲烷的截断值≥4 ppm,或如在一项单机构研究中所述的≥5 ppm,在识别小肠细菌过度生长的10份样本乳果糖呼气测试中基线时会被诊断为“甲烷阳性”的受试者方面都具有高度准确性。