Johnson Mae, Whyte Martin, Loveridge Robert, Yorke Richard, Naleem Shairana
Kings College Hospital, United Kingdom.
BMJ Qual Improv Rep. 2017 Apr 25;6(1). doi: 10.1136/bmjquality.u213254.w6626. eCollection 2017.
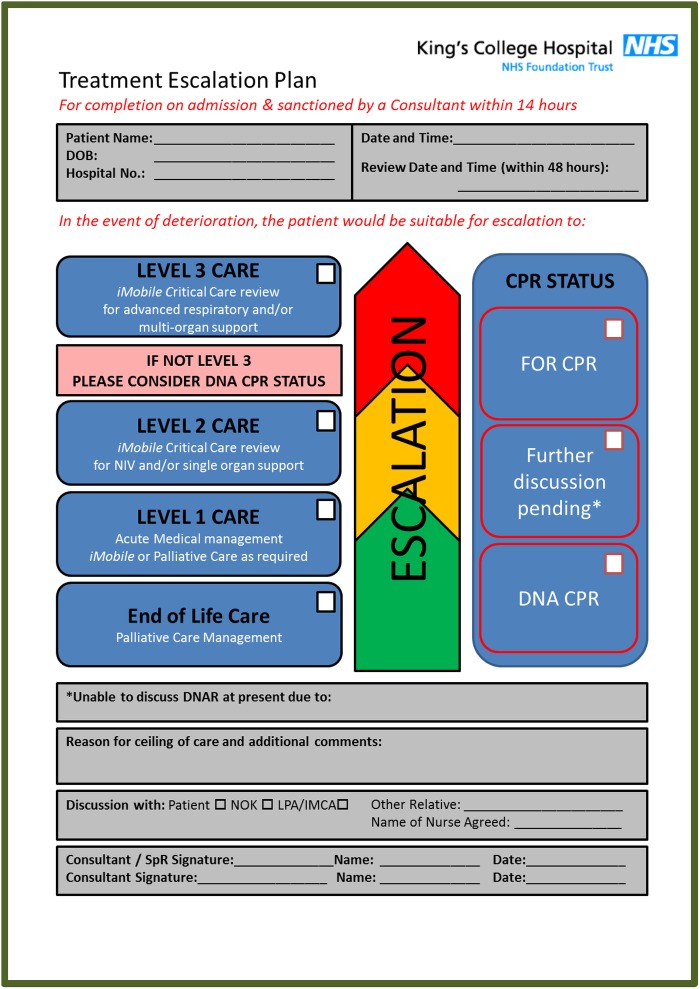
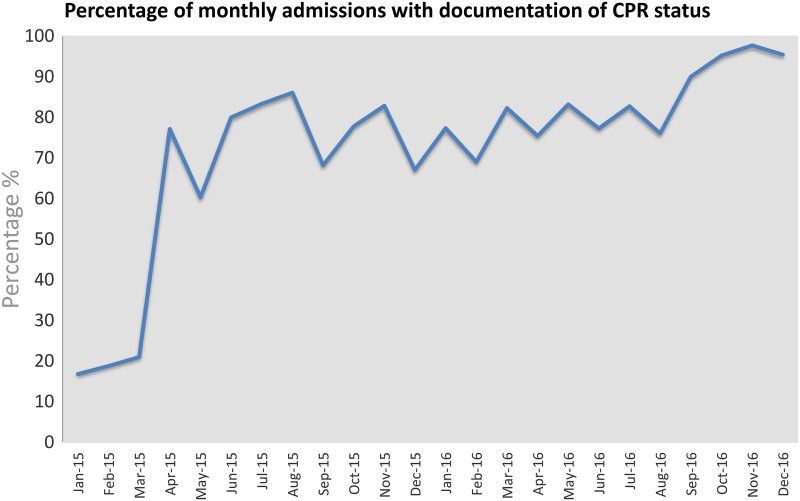
The National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) report 'Time to Intervene' (2012) stated that in a substantial number of cases, resuscitation is attempted when it was thought a 'do not attempt cardiopulmonary resuscitation' (DNACPR) decision should have been in place. Early decisions about CPR status and advance planning about limits of care now form part of national recommendations by the UK Resuscitation Council (2016). Treatment escalation plans (TEP) document what level of treatment intervention would be appropriate if a patient were to become acutely unwell and were not previously formally in place at King's College Hospital. A unifying paper based form was successfully piloted in the Acute Medical Unit, introducing the TEP and bringing together decision making around both treatment escalation and CPR status. Subsequently an electronic order-set for CPR status and treatment escalation was launched in April 2015 which led to a highly visible CPR and escalation status banner on the main screen at the top of the patient's electronic record. Ultimately due to further iterations in the electronic process by December 2016, all escalation decisions for acutely admitted patients now have high quality supporting, explanatory documentation with 100% having TEPs in place. There is now widespread multidisciplinary engagement in the process of defining limits of care for acutely admitted medical patients within the first 14 hours of admission and a strategy for rolling this process out across all the divisions of the hospital through our Deteriorating Patient Group (DPG). The collaborative design with acute medical, palliative and intensive care teams and the high visibility provided by the electronic process in the Electronic Patient Record (EPR) has enhanced communication with these teams, patients, nursing staff and the multidisciplinary team by ensuring clarity through a universally understood process about escalation and CPR. Clarity and openness about these discussions have been welcomed by patient focus groups facilitated via our acute medicine patient experience committee. There has been a shift in medical culture where transparency about limits of care has contributed to improving patient safety and quality of care through reducing unnecessary CPR supported by focus groups of staff.
英国国家患者预后与死亡保密调查(NCEPOD)发布的《干预时机》(2012年)报告指出,在相当多的案例中,当本应做出“不尝试心肺复苏”(DNACPR)决定时,却仍尝试进行复苏。关于心肺复苏状态的早期决策以及对治疗限制的预先规划,现已成为英国复苏委员会(2016年)国家建议的一部分。治疗升级计划(TEP)记录了如果患者病情急剧恶化且此前在国王学院医院未正式制定相关计划时,何种程度的治疗干预是合适的。一种统一的纸质表格在急性医疗单元成功试点,引入了TEP,并将围绕治疗升级和心肺复苏状态的决策整合在一起。随后,2015年4月推出了心肺复苏状态和治疗升级的电子医嘱集,这使得患者电子记录顶部主屏幕上出现了一个非常醒目的心肺复苏和升级状态横幅。最终,由于到2016年12月电子流程的进一步迭代,所有急性入院患者的升级决策现在都有高质量的支持性、解释性文件,100%都有TEP。目前,在急性入院内科患者入院后的前14小时内,界定治疗限制的过程中广泛开展了多学科参与,并且通过我们的病情恶化患者小组(DPG)制定了一项在医院所有科室推广该过程的策略。与急性医疗、姑息治疗和重症监护团队的协作设计以及电子病历(EPR)中电子流程提供的高可见性,通过确保关于升级和心肺复苏的过程被普遍理解而实现清晰透明,从而加强了与这些团队、患者、护理人员和多学科团队的沟通。通过我们的急性医学患者体验委员会促成的患者焦点小组对这些讨论的清晰性和开放性表示欢迎。医疗文化发生了转变,护理限制的透明度通过减少员工焦点小组支持的不必要心肺复苏,有助于提高患者安全和护理质量。