Ghassemi Marzyeh, Wu Mike, Hughes Michael C, Szolovits Peter, Doshi-Velez Finale
Massachusetts Institute of Technology, Cambridge, MA, USA.
Yale University, New Haven, CT, USA.
AMIA Jt Summits Transl Sci Proc. 2017 Jul 26;2017:82-91. eCollection 2017.
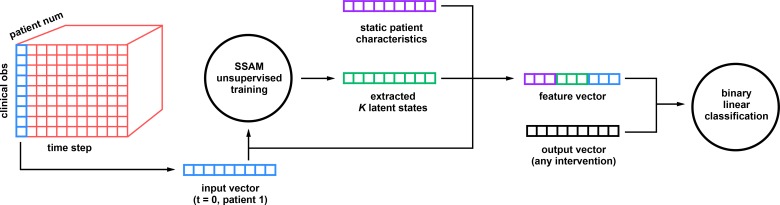
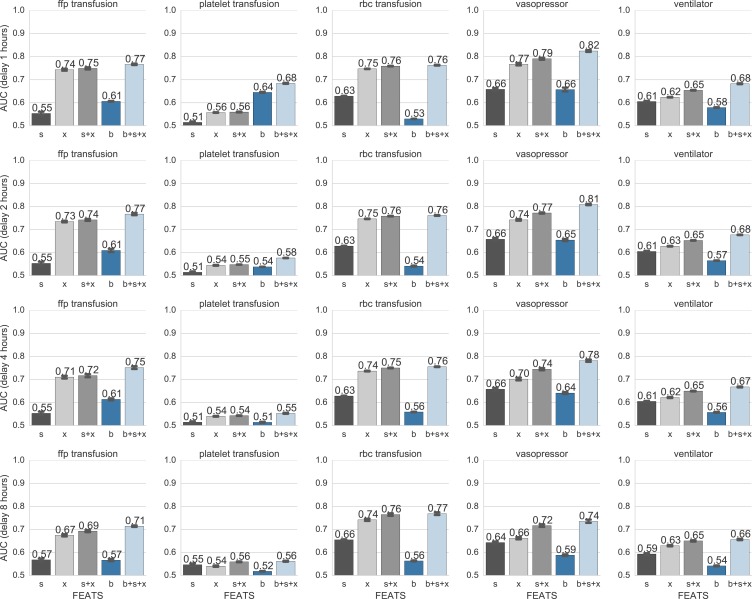
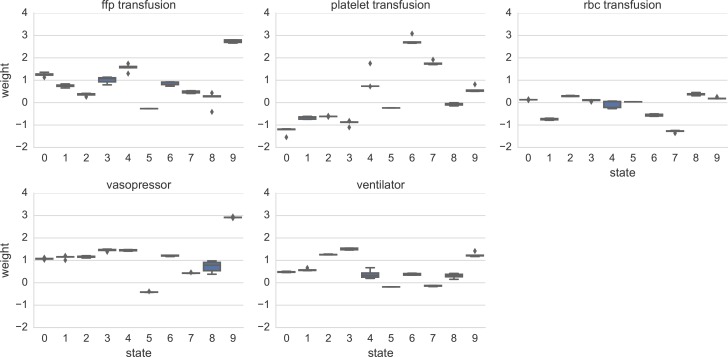
The impact of many intensive care unit interventions has not been fully quantified, especially in heterogeneous patient populations. We train unsupervised switching state autoregressive models on vital signs from the public MIMIC-III database to capture patient movement between physiological states. We compare our learned states to static demographics and raw vital signs in the prediction of five ICU treatments: ventilation, vasopressor administra tion, and three transfusions. We show that our learned states, when combined with demographics and raw vital signs, improve prediction for most interventions even 4 or 8 hours ahead of onset. Our results are competitive with existing work while using a substantially larger and more diverse cohort of 36,050 patients. While custom classifiers can only target a specific clinical event, our model learns physiological states which can help with many interventions. Our robust patient state representations provide a path towards evidence-driven administration of clinical interventions.
许多重症监护病房干预措施的影响尚未得到充分量化,尤其是在异质性患者群体中。我们在公开的MIMIC-III数据库中的生命体征数据上训练无监督切换状态自回归模型,以捕捉患者在生理状态之间的转变。我们将学习到的状态与静态人口统计学数据和原始生命体征进行比较,以预测五种重症监护病房治疗方法:通气、血管加压药给药以及三种输血治疗。我们表明,将我们学习到的状态与人口统计学数据和原始生命体征相结合,即使在治疗开始前4小时或8小时,也能改善对大多数干预措施的预测。我们的结果与现有研究相当,同时使用了一个规模大得多且更加多样化的队列,包含36050名患者。虽然定制分类器只能针对特定的临床事件,但我们的模型学习生理状态,这有助于进行多种干预。我们强大的患者状态表示为临床干预的循证管理提供了一条途径。