Department of General Intensive Care and Institute for Nutrition Research, Rabin Medical Center, Beilinson Hospital, 39 Jabotinsky St, Petah Tikva, Israel.
TSG IT Advanced Systems Ltd., Tel Aviv, Israel.
Sci Rep. 2022 Jun 22;12(1):10573. doi: 10.1038/s41598-022-14758-x.
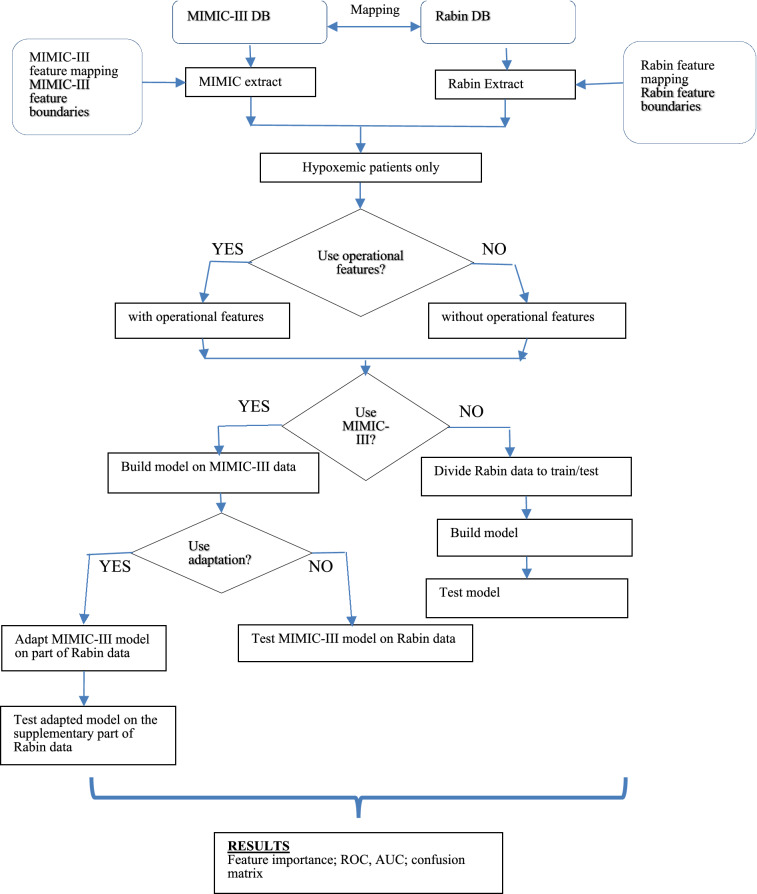
In hypoxemic patients at risk for developing respiratory failure, the decision to initiate invasive mechanical ventilation (IMV) may be extremely difficult, even more so among patients suffering from COVID-19. Delayed recognition of respiratory failure may translate into poor outcomes, emphasizing the need for stronger predictive models for IMV necessity. We developed a two-step model; the first step was to train a machine learning predictive model on a large dataset of non-COVID-19 critically ill hypoxemic patients from the United States (MIMIC-III). The second step was to apply transfer learning and adapt the model to a smaller COVID-19 cohort. An XGBoost algorithm was trained on data from the MIMIC-III database to predict if a patient would require IMV within the next 6, 12, 18 or 24 h. Patients' datasets were used to construct the model as time series of dynamic measurements and laboratory results obtained during the previous 6 h with additional static variables, applying a sliding time-window once every hour. We validated the adaptation algorithm on a cohort of 1061 COVID-19 patients from a single center in Israel, of whom 160 later deteriorated and required IMV. The new XGBoost model for the prediction of the IMV onset was trained and tested on MIMIC-III data and proved to be predictive, with an AUC of 0.83 on a shortened set of features, excluding the clinician's settings, and an AUC of 0.91 when the clinician settings were included. Applying these models "as is" (no adaptation applied) on the dataset of COVID-19 patients degraded the prediction results to AUCs of 0.78 and 0.80, without and with the clinician's settings, respectively. Applying the adaptation on the COVID-19 dataset increased the prediction power to an AUC of 0.94 and 0.97, respectively. Good AUC results get worse with low overall precision. We show that precision of the prediction increased as prediction probability was higher. Our model was successfully trained on a specific dataset, and after adaptation it showed promise in predicting outcome on a completely different dataset. This two-step model successfully predicted the need for invasive mechanical ventilation 6, 12, 18 or 24 h in advance in both general ICU population and COVID-19 patients. Using the prediction probability as an indicator of the precision carries the potential to aid the decision-making process in patients with hypoxemic respiratory failure despite the low overall precision.
在有发生呼吸衰竭风险的低氧血症患者中,是否开始有创机械通气(IMV)的决策可能极其困难,对于 COVID-19 患者更是如此。对呼吸衰竭的识别延迟可能导致不良结局,这强调了需要更强的 IMV 必要性预测模型。我们开发了一个两步模型;第一步是在来自美国的非 COVID-19 危重症低氧血症患者的大型 MIMIC-III 数据集上训练机器学习预测模型。第二步是应用迁移学习并将模型应用于较小的 COVID-19 队列。XGBoost 算法在 MIMIC-III 数据库的数据上进行训练,以预测患者是否会在接下来的 6、12、18 或 24 小时内需要 IMV。使用患者数据集构建模型,将其作为前 6 小时内获得的动态测量和实验室结果的时间序列,并应用滑动时间窗口,每小时应用一次。我们在以色列的一个中心的 1061 例 COVID-19 患者队列上验证了该适应算法,其中 160 例患者病情恶化并需要 IMV。在 MIMIC-III 数据上训练和测试了新的用于预测 IMV 发作的 XGBoost 模型,证明该模型具有预测能力,在缩短的特征集(不包括临床医生的设置)上的 AUC 为 0.83,当包括临床医生的设置时 AUC 为 0.91。在 COVID-19 患者数据集上直接应用这些模型(不进行适应)将预测结果降低至 AUC 分别为 0.78 和 0.80,没有和有临床医生的设置。在 COVID-19 数据集上应用适应后,预测能力分别提高到 AUC 为 0.94 和 0.97。总体精度低时,AUC 结果会变差。我们表明,随着预测概率的提高,预测精度也会提高。我们的模型在特定数据集上成功训练,并且在适应后,它在完全不同的数据集上成功预测了结果。该两步模型成功地预测了普通 ICU 人群和 COVID-19 患者在 6、12、18 或 24 小时内需要有创机械通气的需求。使用预测概率作为精度的指示,有可能在低总体精度的情况下,辅助低氧性呼吸衰竭患者的决策过程。