Moran John L, Santamaria John
Department of Intensive Care Medicine, The Queen Elizabeth Hospital, Woodville, South Australia, Australia.
Department of Critical Care Medicine, St Vincent's Hospital Melbourne, Fitzroy, Victoria, Australia.
PLoS One. 2017 Oct 3;12(10):e0185320. doi: 10.1371/journal.pone.0185320. eCollection 2017.
There has been renewed interest in lactate as a risk biomarker in sepsis and septic shock. However, the ability of the odds ratio (OR) and change in the area under the receiver operator characteristic curve (AUC-ROC) to assess biomarker added-value has been questioned.
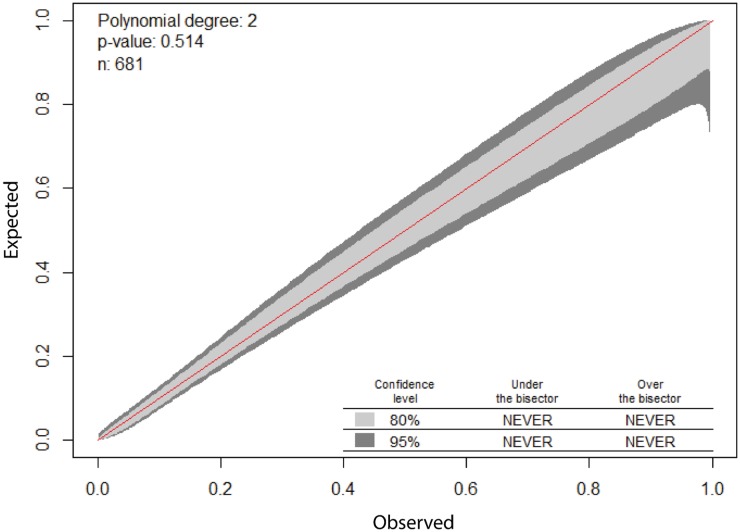
DESIGN, SETTING AND PARTICIPANTS: A sepsis cohort was identified from the ICU database of an Australian tertiary referral hospital using APACHE III diagnostic codes. Demographic information, APACHE III scores, 24-hour post-admission patient lactate levels, and hospital mortality were accessed.
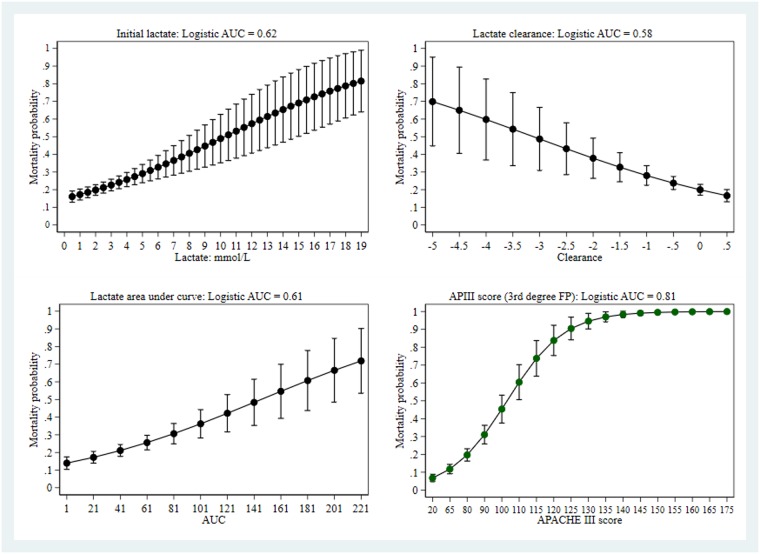
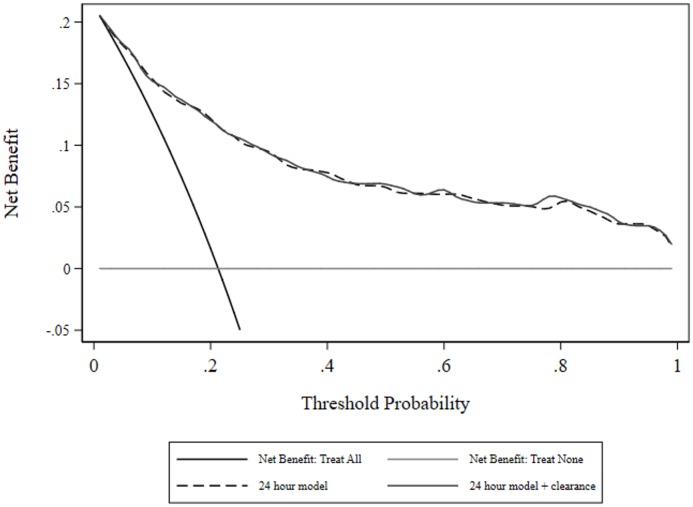
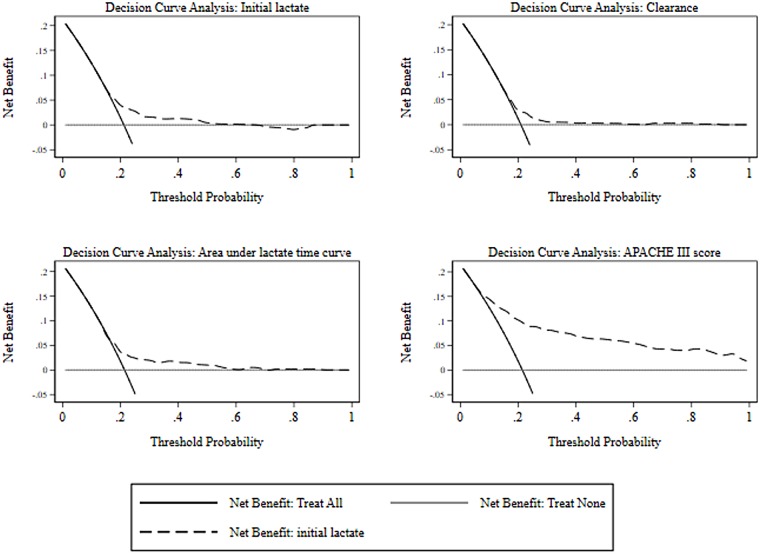
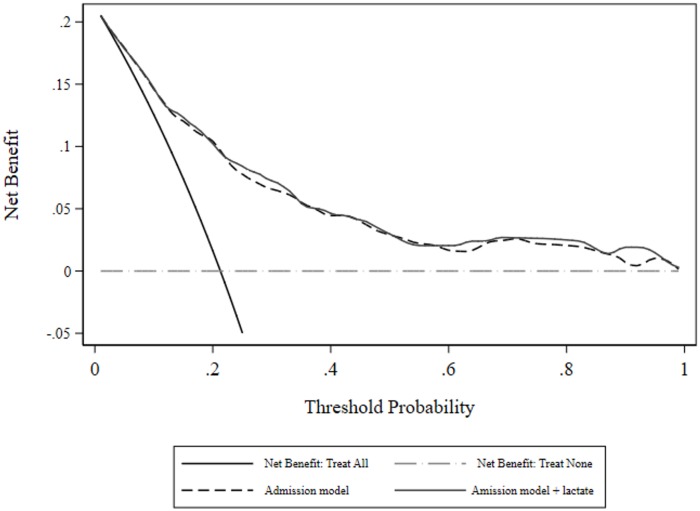
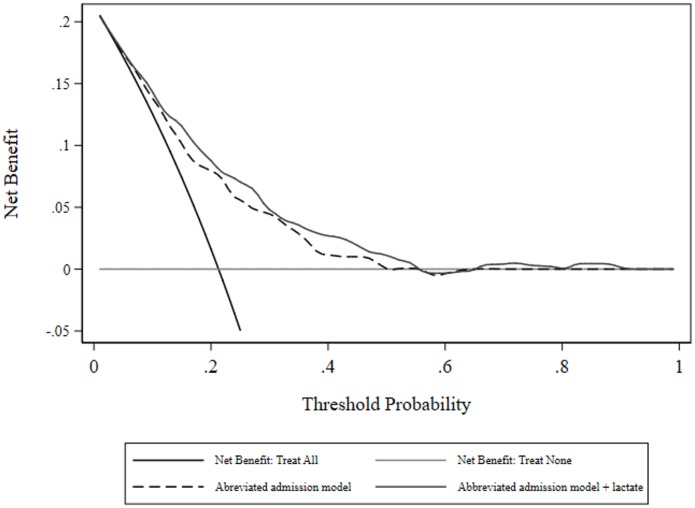
Hospital mortality was modelled using a base predictive logistic regression model and sequential addition of admission lactate, lactate clearance ([lactateadmission-lactatefinal]/lactateadmission), and area under the lactate-time curve (LTC). Added-value was assessed using lactate index OR; AUC-ROC difference (base-model versus lactate index addition); net (mortality) reclassification index (NRI; range -2 to +2); and net benefit (NB), the number of true positives per patient adjusted for the number of false positives. The data set comprised 717 patients with mean(SD) age and APACHE III score 61.1(16.5) years and 68.3(28.2) respectively; 59.2% were male. Admission lactate was 2.3(2.5) mmol/l; with lactate of ≥ 4 mmol/L (37% hospital mortality) in 17% and patients with lactate < 4 mmol/L having 18% hospital mortality. The admission base-model had an AUC-ROC = 0.81 with admission lactate OR = 1.127 (95%CI: 1.038, 1.224), AUC-ROC difference of 0.0032 (-0.0037, 0.01615; P = 0.61), and NRI 0.240(0.030, 0.464). The over-time model had an AUC-ROC = 0.86 with (i) clearance OR = 0.771, 95%CI: 0.578, 1.030; P = 0.08; AUC-ROC difference 0.001 (-0.003, 0.014; P = 0.78), and NRI 0.109(-0.193, 0.425) and (ii) LTC OR = 0.997, 95%CI: 0.989, 1.005, P = 0.49; AUC-ROC difference 0.004 (-0.002, 0.004; P = 0.34), and NRI 0.111(-0.222, 0.403). NB was not incremented by any lactate index.
Lactate added-value assessment is dependent upon the performance of the underlying predictive model and should incorporate risk reclassification and net benefit measures.
乳酸作为脓毒症和脓毒性休克的风险生物标志物再次受到关注。然而,比值比(OR)和受试者工作特征曲线下面积变化(AUC-ROC)评估生物标志物附加值的能力受到了质疑。
设计、设置和参与者:使用APACHE III诊断代码从一家澳大利亚三级转诊医院的重症监护病房数据库中识别出一个脓毒症队列。获取了人口统计学信息、APACHE III评分、入院后24小时患者乳酸水平及医院死亡率。
使用基础预测逻辑回归模型对医院死亡率进行建模,并依次加入入院乳酸、乳酸清除率([入院乳酸-最终乳酸]/入院乳酸)和乳酸-时间曲线下面积(LTC)。使用乳酸指数OR评估附加值;AUC-ROC差异(基础模型与加入乳酸指数后的模型);净(死亡率)重新分类指数(NRI;范围-2至+2);以及净效益(NB),即根据假阳性数量调整后的每位患者真阳性数量。数据集包括717例患者,平均(标准差)年龄和APACHE III评分分别为61.1(16.5)岁和68.3(28.2);59.2%为男性。入院乳酸水平为2.3(2.5)mmol/L;17%的患者乳酸≥4 mmol/L(医院死亡率37%),乳酸<4 mmol/L的患者医院死亡率为18%。入院基础模型的AUC-ROC = 0.81,入院乳酸OR = 1.127(95%CI:1.038,1.224),AUC-ROC差异为0.0032(-0.0037,0.01615;P = 0.61),NRI为0.240(0.030,0.464)。随时间变化的模型AUC-ROC = 0.86,(i)清除率OR = 0.771,95%CI:0.578,1.030;P = 0.08;AUC-ROC差异0.001(-0.003,0.014;P = 0.78),NRI为0.109(-0.193,0.425),以及(ii)LTC OR = 0.997,95%CI:0.989,1.005,P = 0.49;AUC-ROC差异0.004(-0.002,0.004;P = 0.34),NRI为0.111(-0.222,0.403)。任何乳酸指数均未增加NB。
乳酸附加值评估取决于基础预测模型的性能,应纳入风险重新分类和净效益测量。