Brummel Nathan E, Boehm Leanne M, Girard Timothy D, Pandharipande Pratik P, Jackson James C, Hughes Christopher G, Patel Mayur B, Han Jin H, Vasilevskis Eduard E, Thompson Jennifer L, Chandrasekhar Rameela, Bernard Gordon R, Dittus Robert S, Ely E Wesley
Nathan E. Brummel is an assistant professor and E. Wesley Ely is a professor, Department of Medicine, Center for Quality Aging and the Center for Health Services Research, Vanderbilt University Medical Center, Nashville, Tennessee. Dr Ely is also the associate director for research for the Geriatric Research, Education, and Clinical Center Service (GRECC), Department of Veterans Affairs Medical Center, Tennessee Valley Healthcare System, Nashville, Tennessee. Leanne M. Boehm is a postdoctoral fellow, Vanderbilt University School of Nursing, a quality scholar, GRECC, Department of Veterans Affairs Medical Center, Tennessee Valley Healthcare System, and a research nurse, Department of Medicine, Center for Health Services Research, Vanderbilt University Medical Center. Timothy D. Girard is an associate professor, Clinical Research, Investigation, and Systems Modeling of Acute Illness Center, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania. Pratik P. Pandharipande is a professor and Christopher G. Hughes is an associate professor, Department of Anesthesiology, Vanderbilt University Medical Center. James C. Jackson is a research associate professor, Department of Medicine, Department of Psychiatry and Behavioral Sciences, Vanderbilt University Medical Center, and Mayur B. Patel is an assistant professor, Department of Surgery, Vanderbilt University Medical Center. Jin H. Han is an associate professor, Department of Emergency Medicine and Center for Quality Aging, Vanderbilt University Medical Center. Eduard E. Vasilevskis is a staff physician, GRECC, Department of Veterans Affairs Medical Center, VA Tennessee Valley Healthcare System, and an assistant professor, Department of Medicine and Center for Health Services Research, Vanderbilt University Medical Center. Jennifer L. Thompson is a biostatistician and Rameela Chandrasekhar is an assistant professor, Department of Biostatistics, Vanderbilt University School of Medicine. Gordon R. Bernard is associate vice-chancellor for research and a professor, Department of Medicine, Vanderbilt University Medical Center. Robert S. Dittus is director, GRECC, Department of Veterans Affairs Medical Center, VA Tennessee Valley Healthcare System, and a professor, Department of Medicine, Vanderbilt University Medical Center.
Am J Crit Care. 2017 Nov;26(6):447-455. doi: 10.4037/ajcc2017263.
The prognostic importance of subsyndromal delirium is unknown.
To test whether duration of subsyndromal delirium is independently associated with institutionalization.
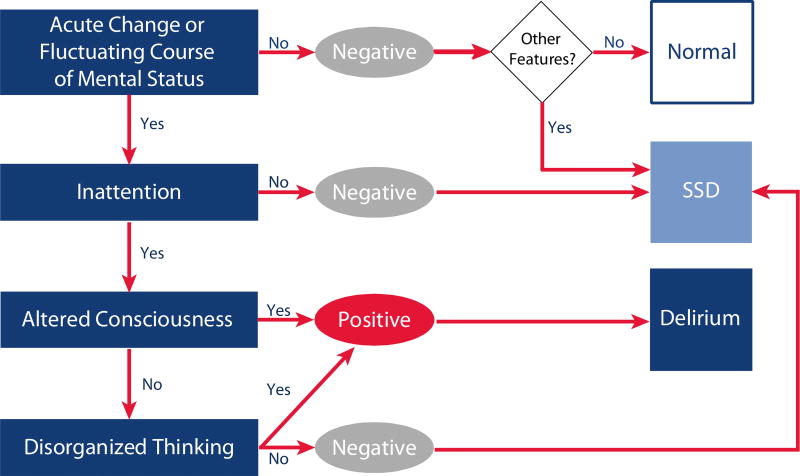
The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) was used twice daily to assess for subsyndromal delirium in patients with respiratory failure or shock. Delirium was considered present if the assessment was positive. Subsyndromal delirium was considered present if the assessment was negative but the patient exhibited any CAM-ICU features. Multivariable regression was used to determine the association between duration of subsyndromal delirium and institutionalization, adjusting for age, education, baseline cognition and disability, comorbidities, severity of illness, delirium, coma, sepsis, and doses of sedatives and opiates.
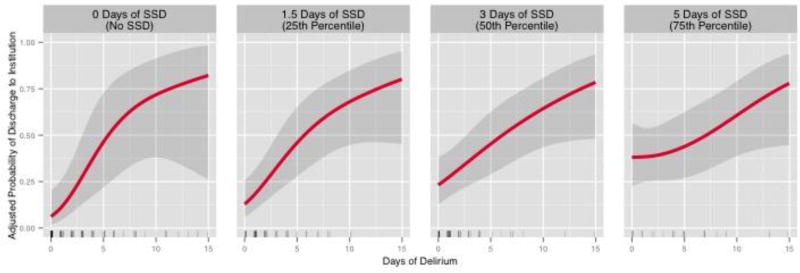
Subsyndromal delirium, lasting a median of 3 days, developed in 702 of 821 patients (86%). After adjusting for covariates, duration of subsyndromal delirium was an independent predictor of increased odds of institutionalization ( = .007). This association was greatest in patients with less delirium ( for interaction = .01). Specifically, of patients who were never delirious, those with 5 days of subsyndromal delirium (upper interquartile range [IQR]) were 4.2 times more likely to be institutionalized than those with 1.5 days of subsyndromal delirium (lower IQR).
Subsyndromal delirium occurred in most critically ill patients, and its duration was an independent predictor of institutionalization. Routine monitoring of all delirium symptoms may enable detection of full and subsyndromal forms of delirium.
亚综合征性谵妄的预后重要性尚不清楚。
检验亚综合征性谵妄的持续时间是否与入住养老院独立相关。
采用重症监护病房意识模糊评估法(CAM-ICU)每天对呼吸衰竭或休克患者进行两次评估,以检测亚综合征性谵妄。如果评估结果为阳性,则认为存在谵妄。如果评估结果为阴性,但患者表现出任何CAM-ICU特征,则认为存在亚综合征性谵妄。采用多变量回归分析确定亚综合征性谵妄持续时间与入住养老院之间的关联,并对年龄、教育程度、基线认知和残疾情况、合并症、疾病严重程度、谵妄、昏迷、脓毒症以及镇静剂和阿片类药物剂量进行校正。
821例患者中有702例(86%)出现了亚综合征性谵妄,持续时间中位数为3天。校正协变量后,亚综合征性谵妄的持续时间是入住养老院几率增加的独立预测因素(P = 0.007)。这种关联在谵妄程度较轻的患者中最为明显(交互作用P = 0.01)。具体而言,在从未发生谵妄的患者中,亚综合征性谵妄持续5天(上四分位数间距[IQR])的患者入住养老院的可能性是亚综合征性谵妄持续1.5天(下IQR)患者的4.2倍。
大多数重症患者会出现亚综合征性谵妄,其持续时间是入住养老院的独立预测因素。对所有谵妄症状进行常规监测可能有助于发现谵妄的完全形式和亚综合征形式。