Nutritional Epidemiology Group (NEG), School of Food Science and Nutrition, University of Leeds, Leeds LS2 9JT, UK.
Division of Noncommunicable Diseases and Promoting Health through the Life-Course, World Health Organization Regional Office for Europe, UN City, Marmorvej 51, DK-2100 Copenhagen, Denmark.
Nutrients. 2017 Nov 27;9(12):1288. doi: 10.3390/nu9121288.
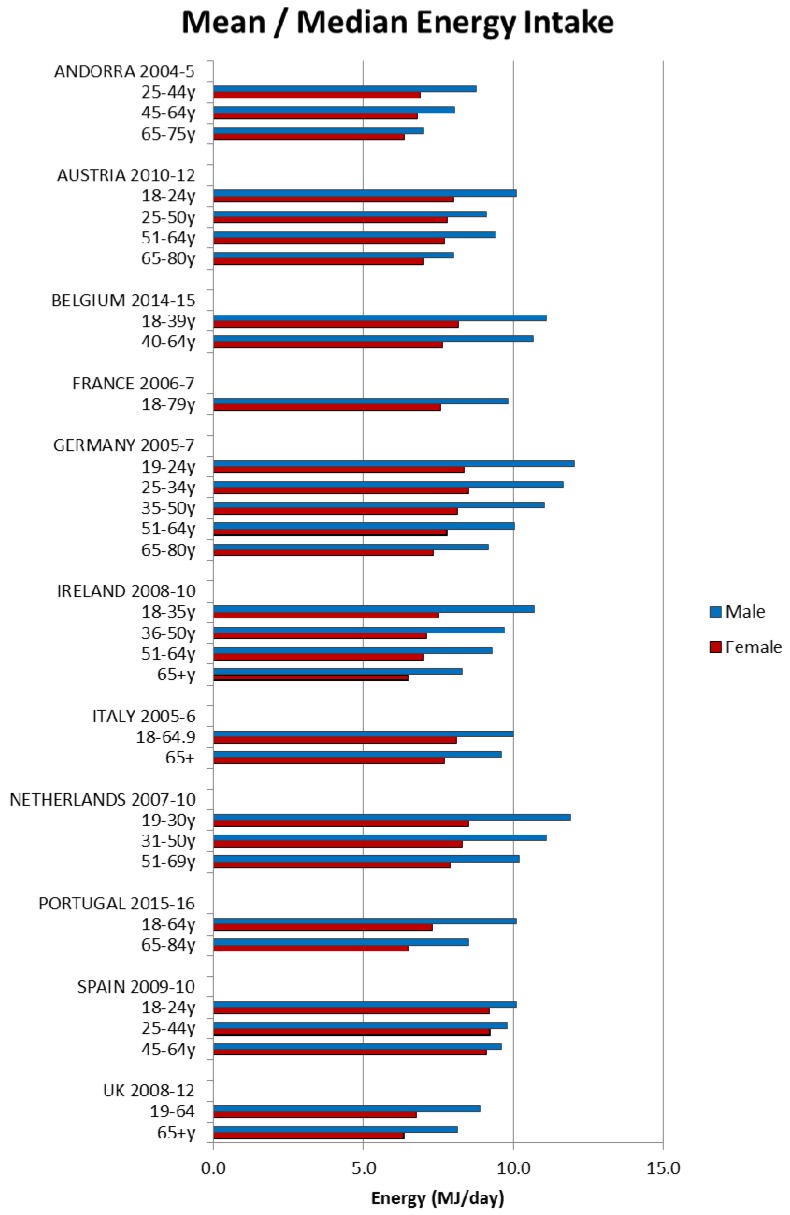
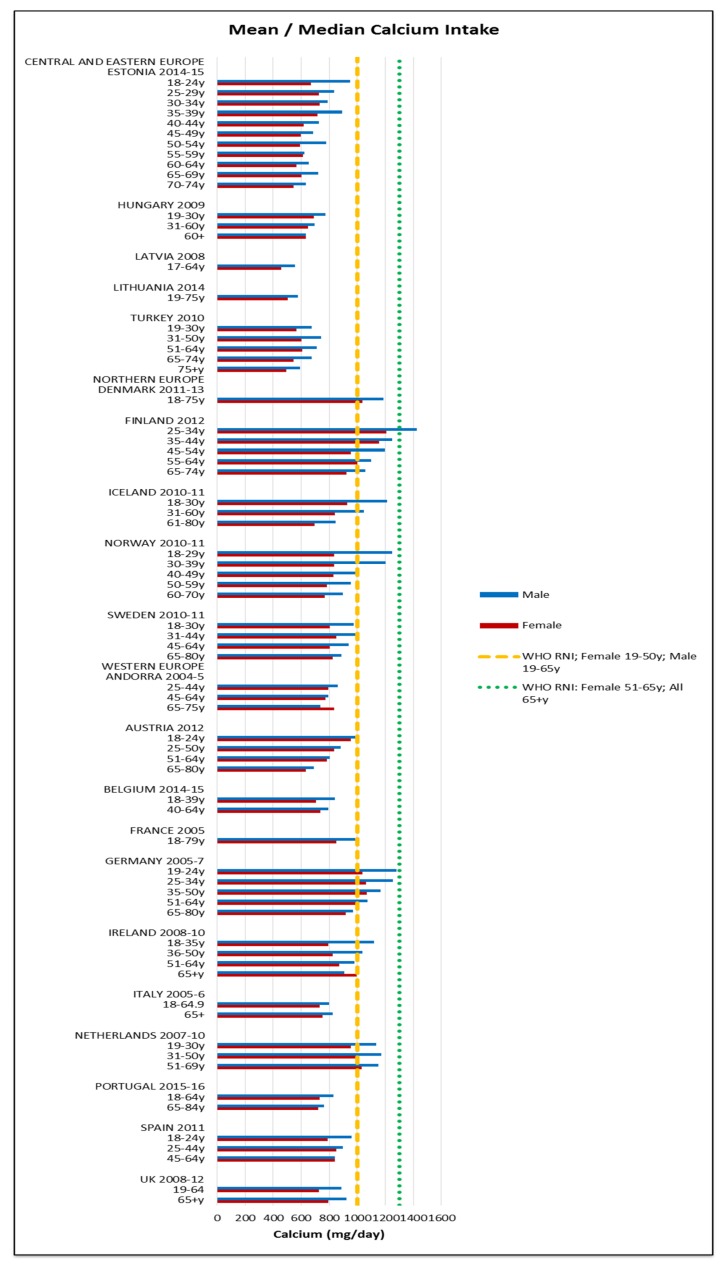
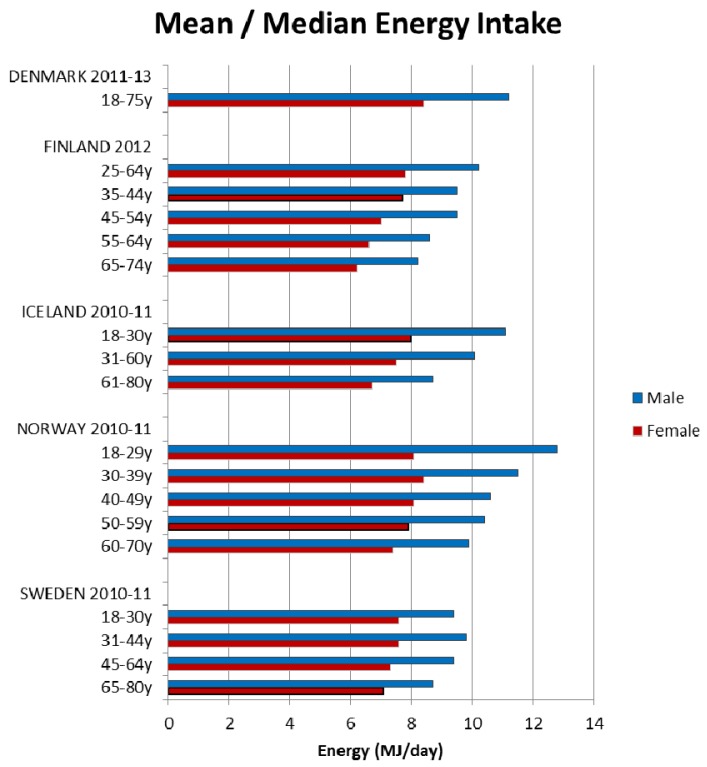
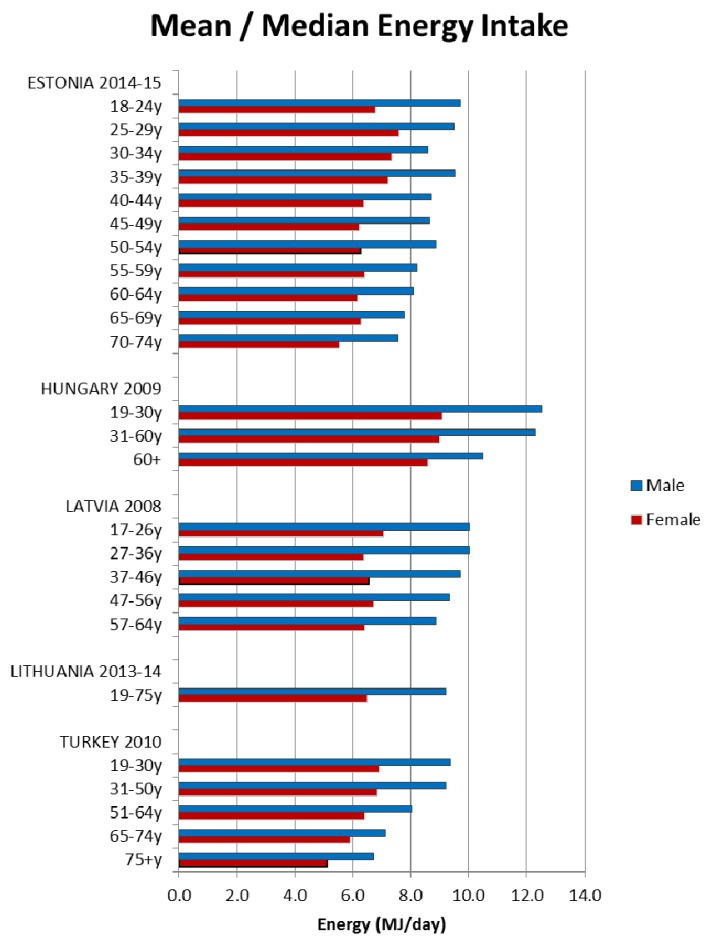
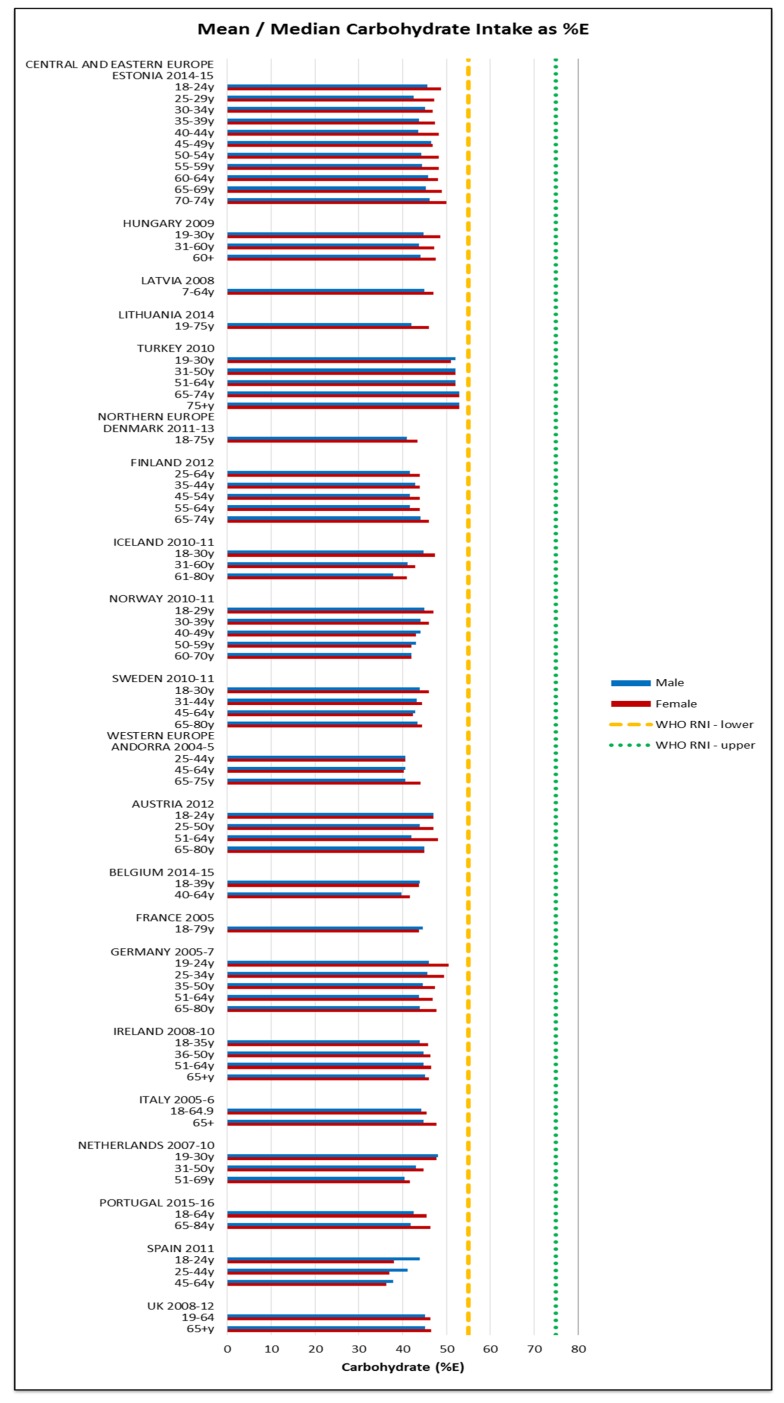
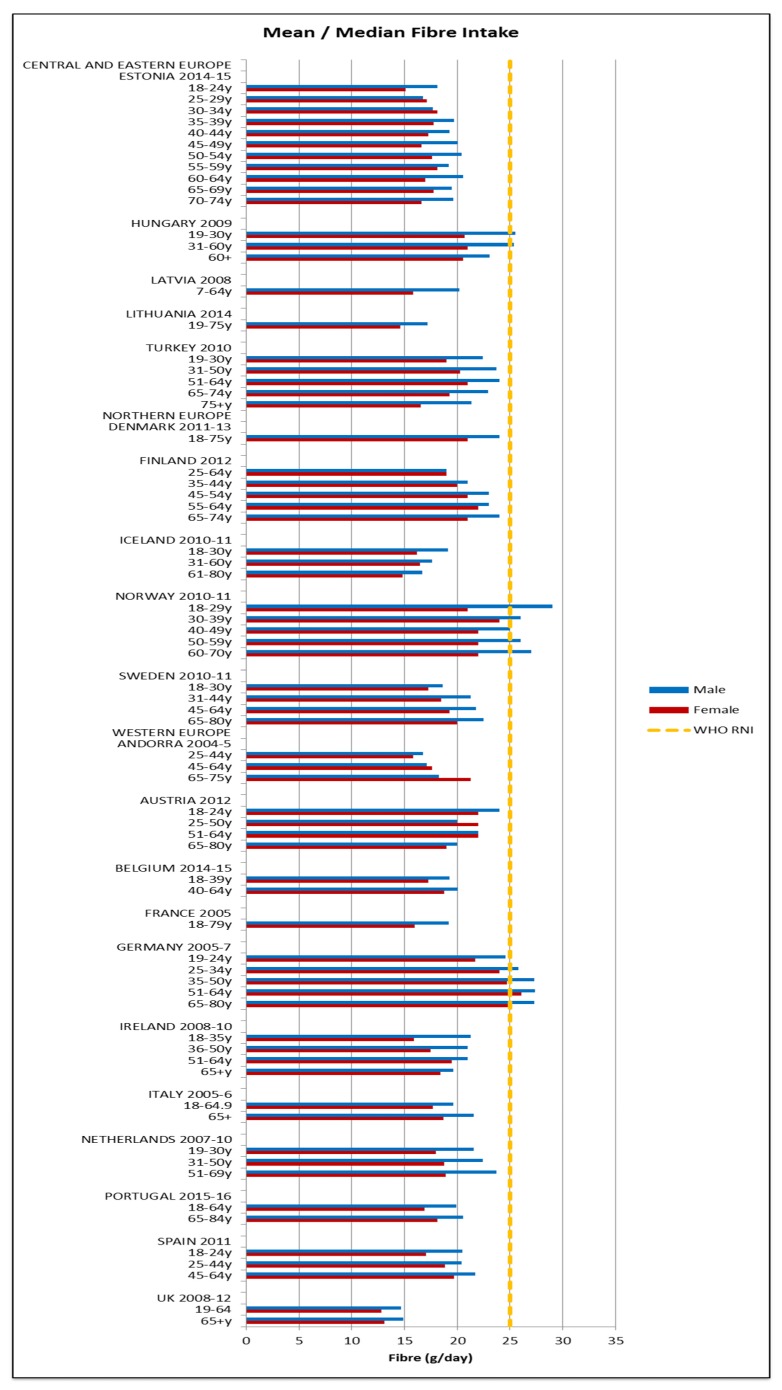
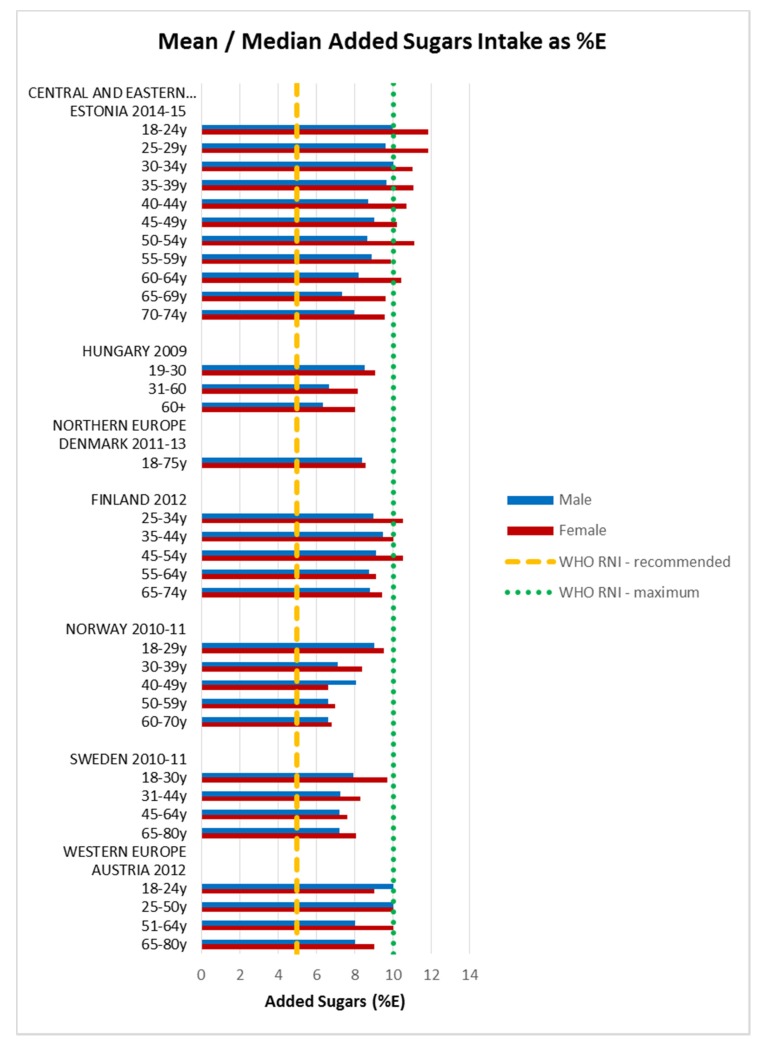
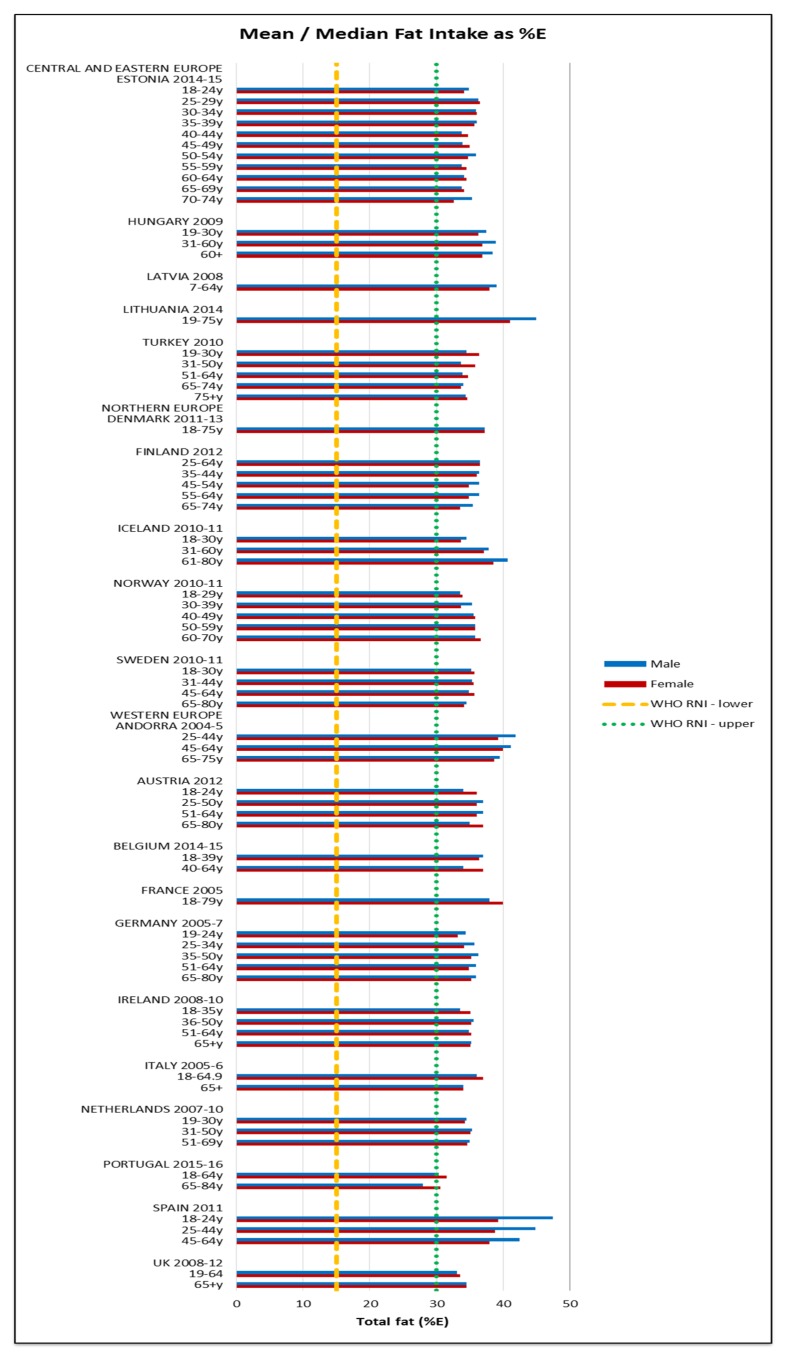
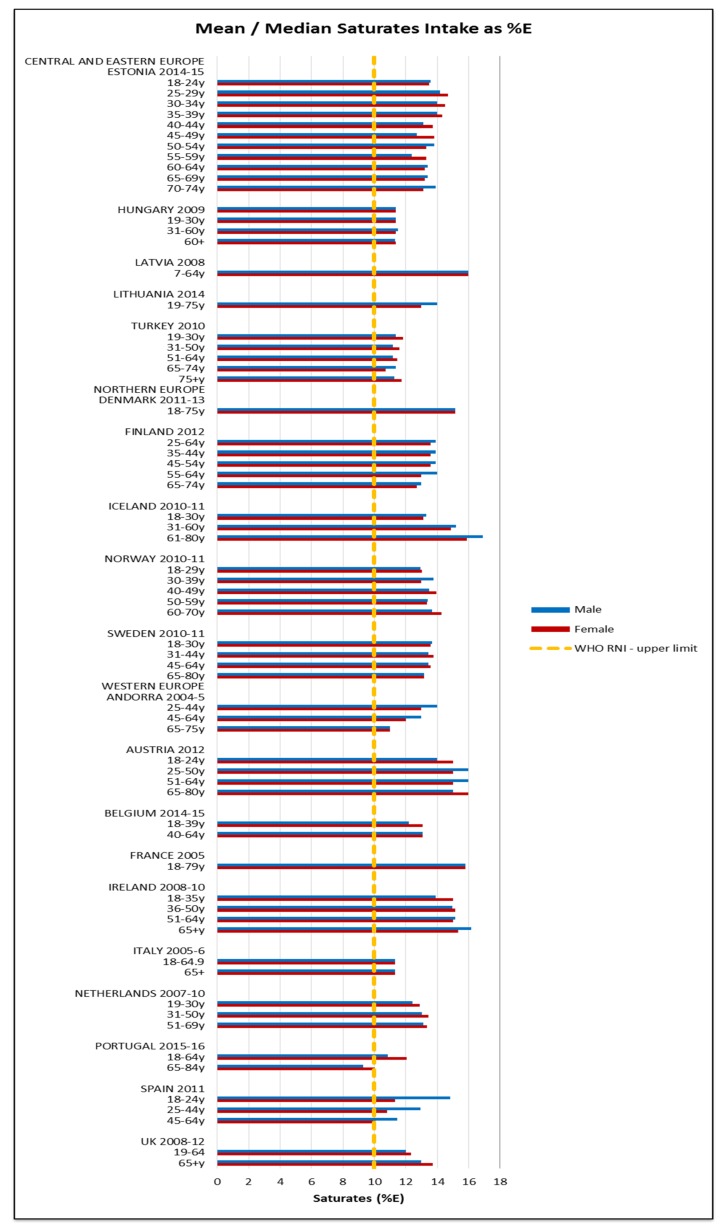
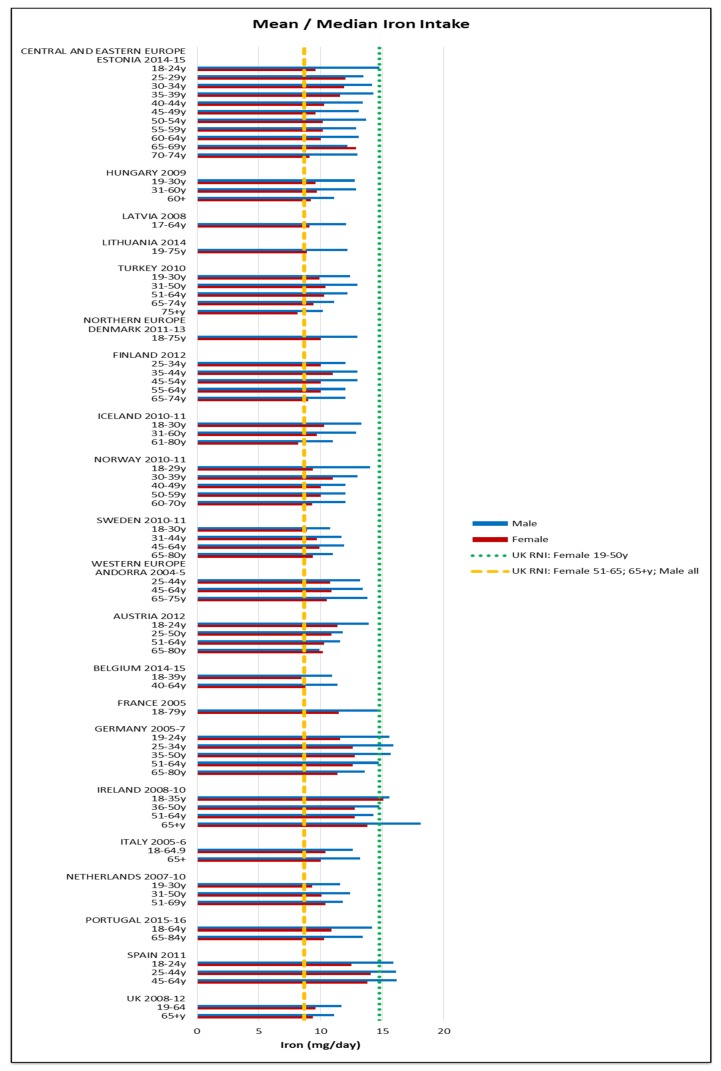
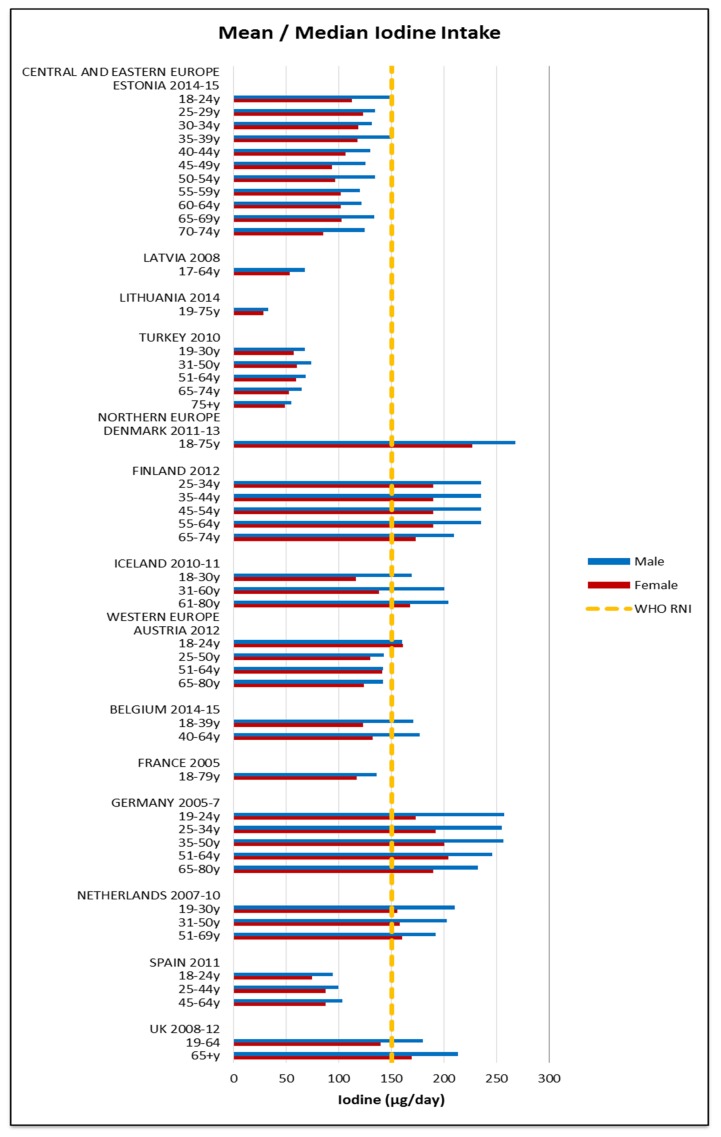
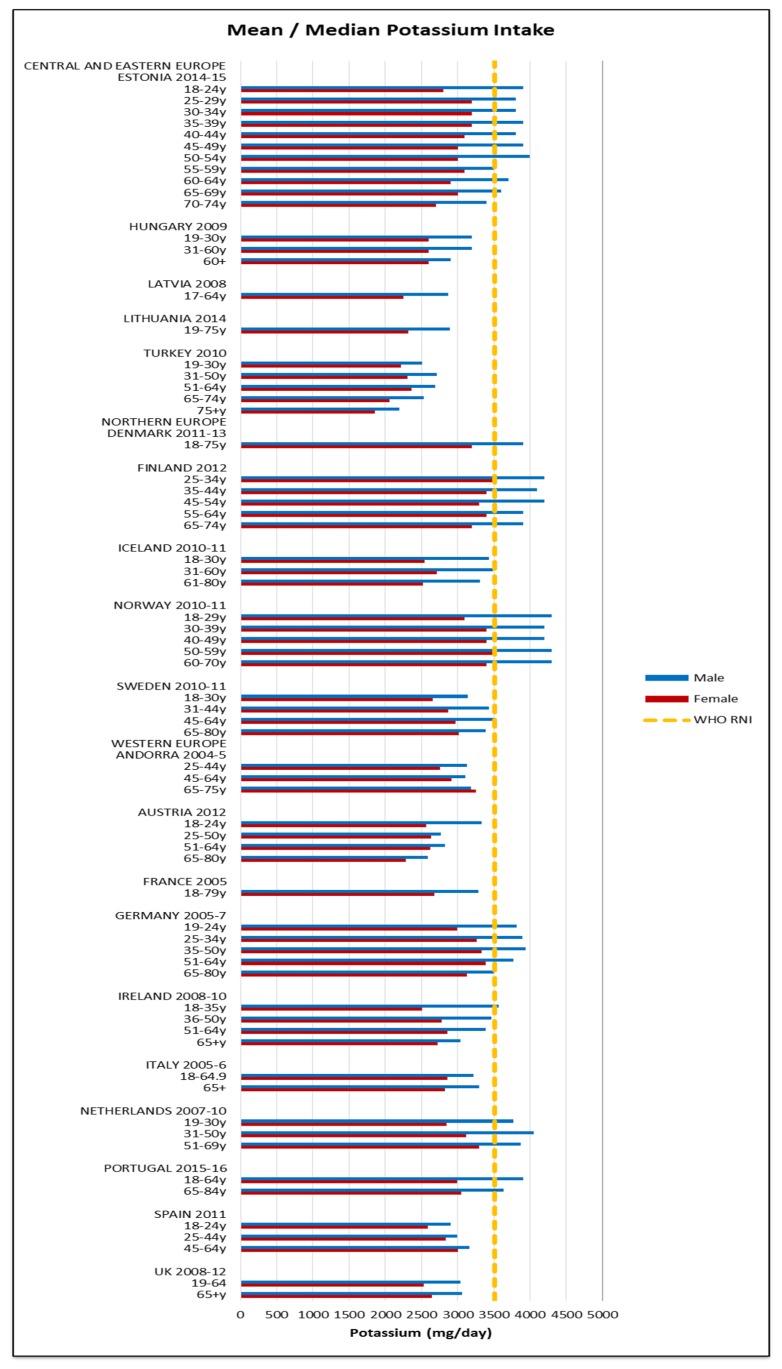
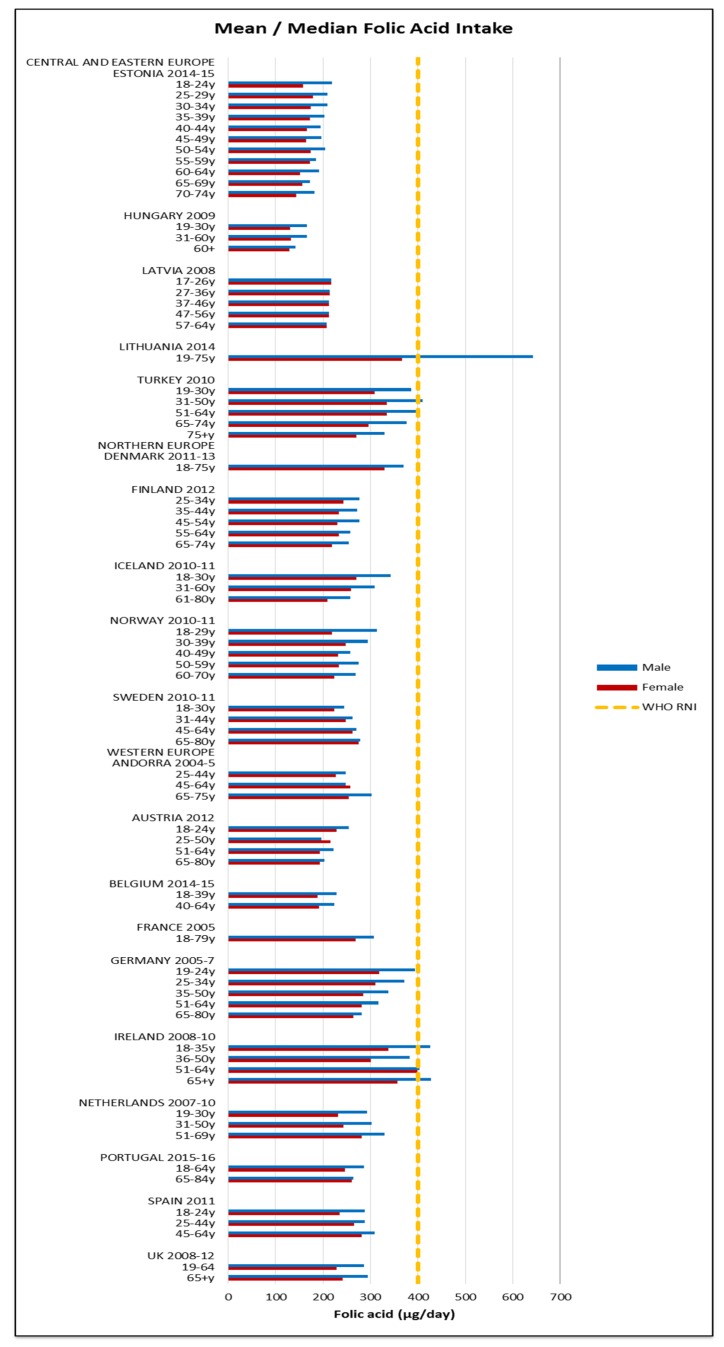
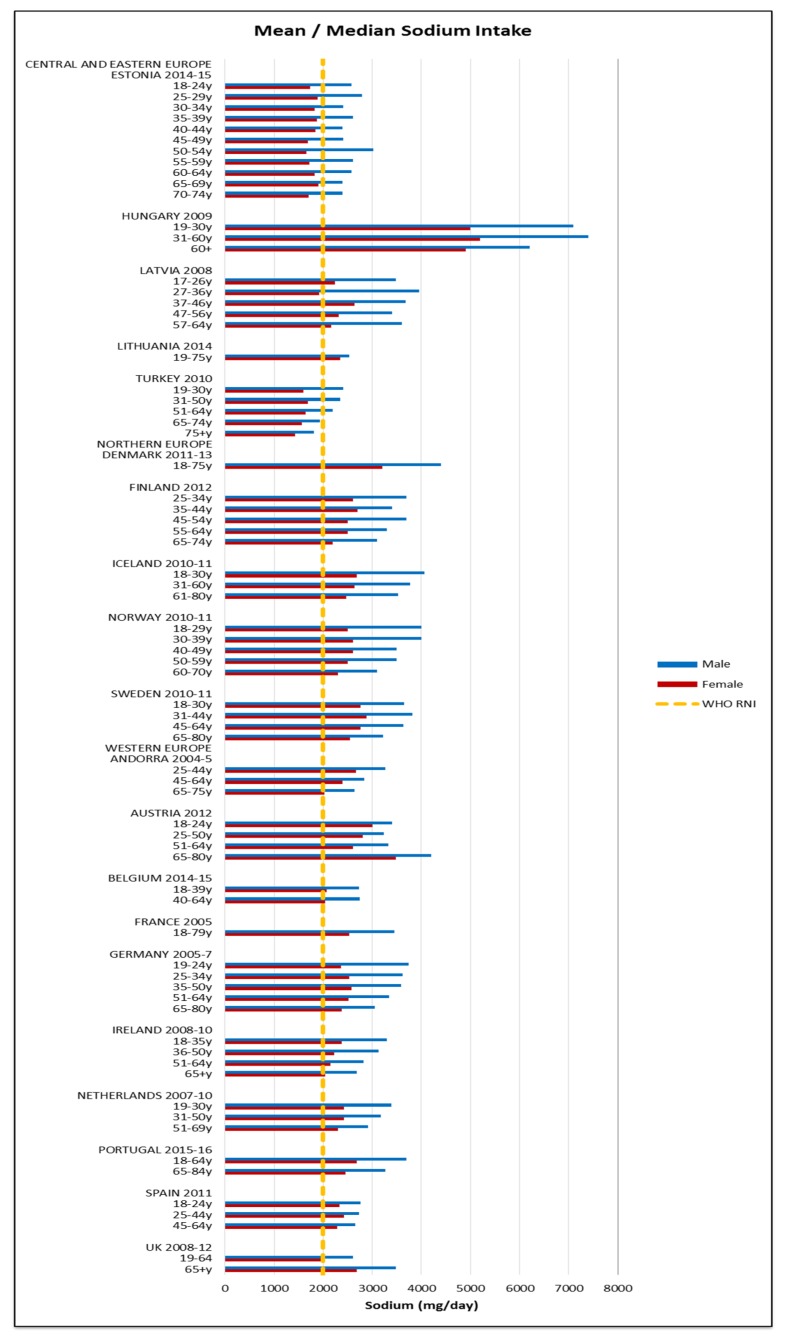
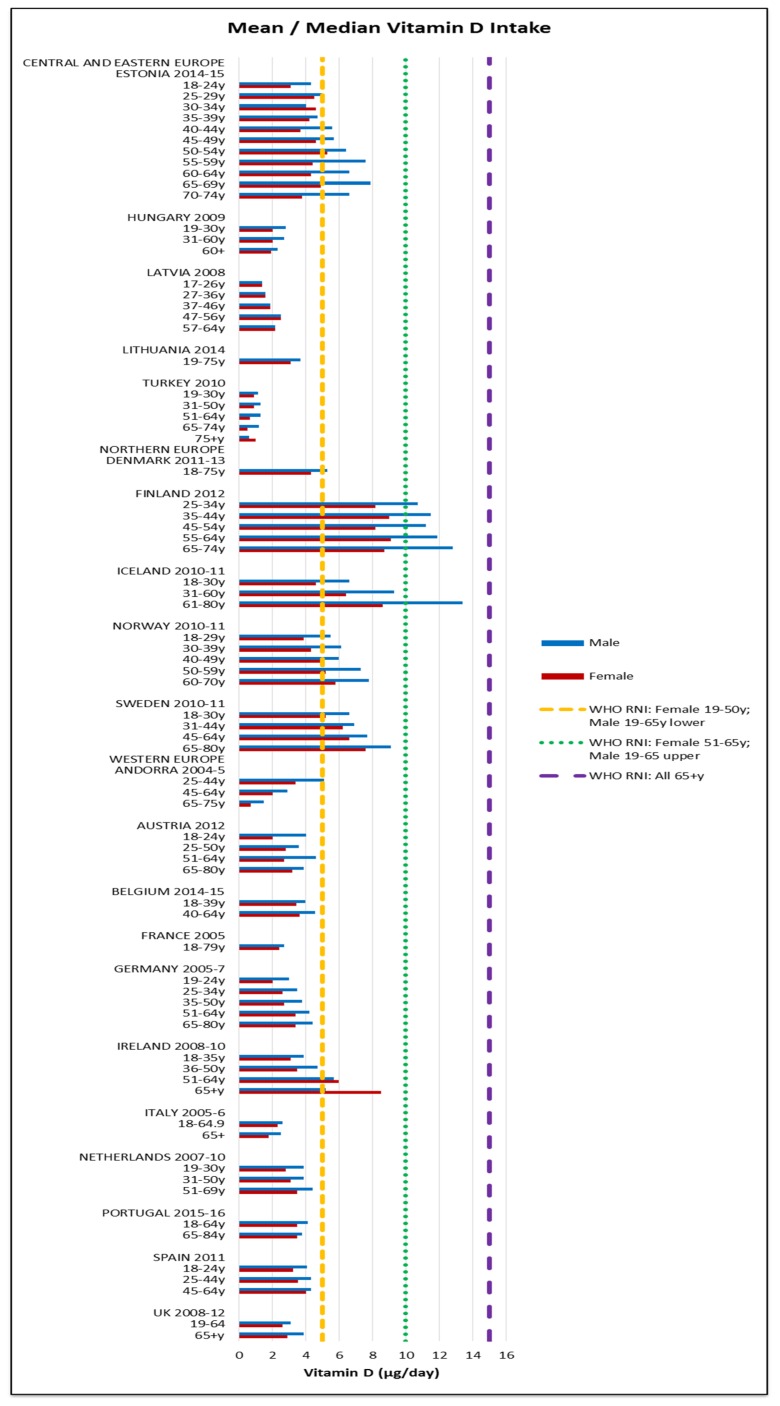
The World Health Organization (WHO) encourages countries to undertake national dietary survey (NDS) but implementation and reporting is inconsistent. This paper provides an up-to-date review of adult macro and micronutrient intakes in European populations as reported by NDS. It uses WHO Recommended Nutrient Intakes (RNIs) to assess intake adequacy and highlight areas of concern. NDS information was gathered primarily by internet searches and contacting survey authors and nutrition experts. Survey characteristics and adult intakes by gender/age group were extracted for selected nutrients and weighted means calculated by region. Of the 53 WHO Europe countries, over a third ( = 19), mainly Central & Eastern European countries (CEEC), had no identifiable NDS. Energy and nutrient intakes were extracted for 21 (40%) countries but differences in age group, methodology, under-reporting and nutrient composition databases hindered inter-country comparisons. No country met more than 39% WHO RNIs in all age/gender groups; macronutrient RNI achievement was poorer than micronutrient. Overall RNI attainment was slightly worse in CEEC and lower in women and female elderly. Only 40% countries provided adult energy and nutrient intakes. The main gaps lie in CEEC, where unknown nutrient deficiencies may occur. WHO RNI attainment was universally poor for macronutrients, especially for women, the female elderly and CEEC. All countries could be encouraged to report a uniform nutrient set and sub-analyses of nationally representative nutrient intakes.
世界卫生组织(WHO)鼓励各国开展国家饮食调查(NDS),但实施和报告情况不一致。本文最新综述了欧洲人群的成人宏观和微量营养素摄入量,这些数据来自 NDS 报告。本文使用世界卫生组织推荐的营养素摄入量(RNIs)评估摄入量是否充足,并强调需要关注的领域。NDS 信息主要通过互联网搜索以及联系调查作者和营养专家收集。针对选定的营养素,提取了调查特征和按性别/年龄组划分的成人摄入量,并按地区计算加权平均值。在 53 个世卫组织欧洲成员国中,超过三分之一(=19 个),主要是中东欧和东欧国家(CEEC),没有可识别的 NDS。有 21 个(40%)国家提取了能量和营养素摄入量,但由于年龄组、方法、低报和营养素组成数据库的差异,阻碍了国家间的比较。没有一个国家在所有年龄/性别组都达到了超过 39%的世卫组织 RNIs;宏量营养素的 RNI 实现情况不如微量营养素。CEEC 的整体 RNI 达标情况略差,女性和老年女性的情况更差。只有 40%的国家提供了成人的能量和营养素摄入量。主要的差距存在于 CEEC,这些国家可能存在未知的营养缺乏。对于宏量营养素,尤其是对于女性、老年女性和 CEEC,世卫组织 RNI 的达标情况普遍较差。所有国家都可以鼓励报告统一的营养素组和全国代表性营养素摄入量的亚分析。