van Andel Judith, Ungureanu Constantin, Arends Johan, Tan Francis, Van Dijk Johannes, Petkov George, Kalitzin Stiliyan, Gutter Thea, de Weerd Al, Vledder Ben, Thijs Roland, van Thiel Ghislaine, Roes Kit, Leijten Frans
Department of Neurology Brain Center Rudolf Magnus University Medical Center Utrecht Utrecht the Netherlands.
Academic Center for Epileptology Epilepsy Center Kempenhaeghe Heeze the Netherlands.
Epilepsia Open. 2017 Sep 6;2(4):424-431. doi: 10.1002/epi4.12076. eCollection 2017 Dec.
Automated seizure detection and alarming could improve quality of life and potentially prevent sudden, unexpected death in patients with severe epilepsy. As currently available systems focus on tonic-clonic seizures, we want to detect a broader range of seizure types, including tonic, hypermotor, and clusters of seizures.
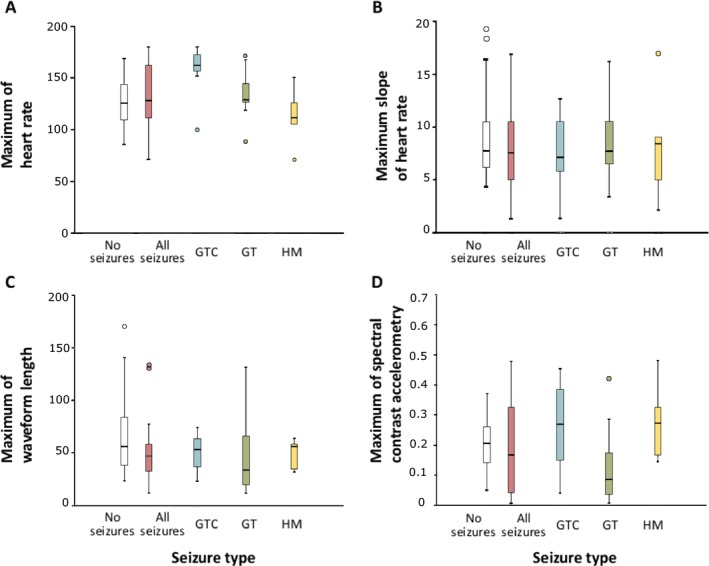
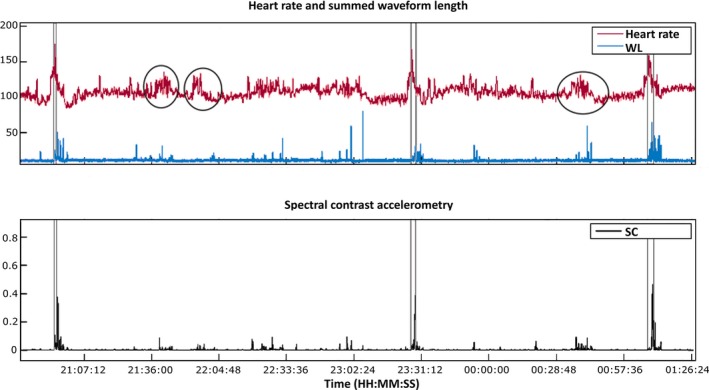
In this multicenter, prospective cohort study, the nonelectroencephalographic (non-EEG) signals heart rate and accelerometry were measured during the night in patients undergoing a diagnostic video-EEG examination. Based on clinical video-EEG data, seizures were classified and categorized as clinically urgent or not. Seizures included for analysis were tonic, tonic-clonic, hypermotor, and clusters of short myoclonic/tonic seizures. Features reflecting physiological changes in heart rate and movement were extracted. Detection algorithms were developed based on stepwise fulfillment of conditions during increases in either feature. A training set was used for development of algorithms, and an independent test set was used for assessing performance.
Ninety-five patients were included, but due to sensor failures, data from only 43 (of whom 23 patients had 86 seizures, representing 402 h of data) could be used for analysis. The algorithms yield acceptable sensitivities, especially for clinically urgent seizures (sensitivity = 71-87%), but produce high false alarm rates (2.3-5.7 per night, positive predictive value = 25-43%). There was a large variation in the number of false alarms per patient.
It seems feasible to develop a detector with high sensitivity, but false alarm rates are too high for use in clinical practice. For further optimization, personalization of algorithms may be necessary.
自动癫痫发作检测与报警可改善生活质量,并有可能预防严重癫痫患者的突然意外死亡。由于目前可用的系统主要关注强直阵挛性发作,我们希望检测更广泛的癫痫发作类型,包括强直发作、多动性发作和发作簇。
在这项多中心前瞻性队列研究中,对接受诊断性视频脑电图检查的患者在夜间测量非脑电图(非EEG)信号心率和加速度。根据临床视频脑电图数据,将癫痫发作分类并归类为临床紧急或非紧急。纳入分析的癫痫发作类型包括强直发作、强直阵挛性发作、多动性发作和短阵性肌阵挛/强直发作簇。提取反映心率和运动生理变化的特征。基于任一特征增加时条件的逐步满足开发检测算法。使用训练集开发算法,使用独立测试集评估性能。
纳入95例患者,但由于传感器故障,仅43例患者(其中23例患者有86次发作,代表402小时的数据)的数据可用于分析。这些算法产生了可接受的敏感性,特别是对于临床紧急发作(敏感性=71-87%),但产生了较高的误报率(每晚2.3-5.7次,阳性预测值=25-43%)。每位患者的误报次数差异很大。
开发具有高敏感性的检测器似乎是可行的,但误报率过高,无法用于临床实践。为了进一步优化,可能需要对算法进行个性化。