Cochrane South Africa, South African Medical Research Council, Cape Town, South Africa.
European and Developing Countries Clinical Trial Partnership (EDCTP), Cape Town, South Africa.
PLoS One. 2018 Mar 30;13(3):e0195025. doi: 10.1371/journal.pone.0195025. eCollection 2018.
Agreed international development standards underpin high quality de novo clinical practice guidelines (CPGs). There is however, no international consensus on how high quality CPGs should 'look'; or on whether high quality CPGs from one country can be viably implemented elsewhere. Writing de novo CPGs is generally resource-intensive and expensive, making this challenging in resource-poor environments. This paper proposes an alternative, efficient method of producing high quality CPGs in such circumstances, using existing CPGs layered by local knowledge, contexts and products.
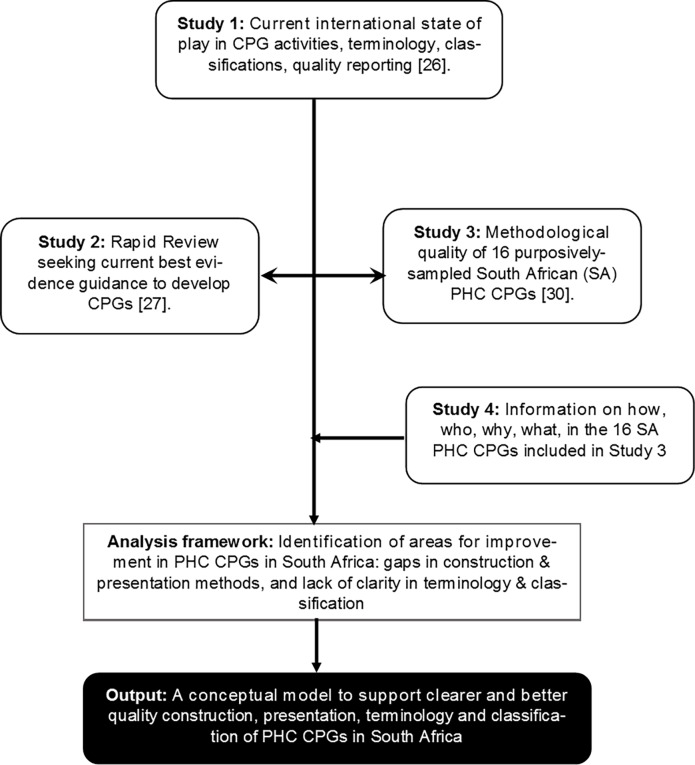
We undertook a mixed methods case study in South African (SA) primary healthcare (PHC), building on findings from four independent studies. These comprised an overview of international CPG activities; a rapid literature review on international CPG development practices; critical appraisal of 16 purposively-sampled SA PHC CPGs; and additional interrogation of these CPGs regarding how, why and for whom, they had been produced, and how they 'looked'.
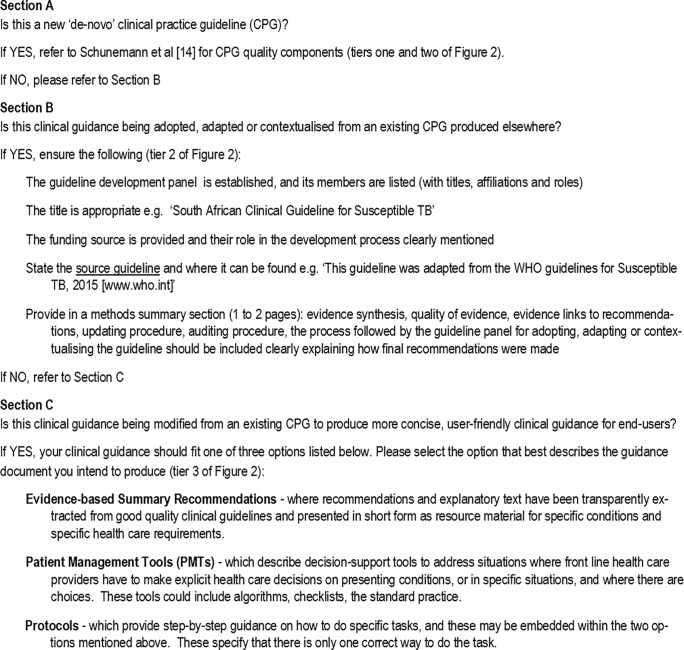
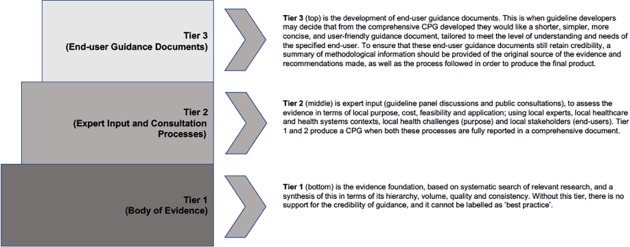
Despite a common aim to improve SA PHC healthcare practices, the included CPGs had different, unclear and inconsistent production processes, terminology and evidence presentation styles. None aligned with international quality standards. However many included innovative succinct guidance for end-users (which we classified as evidence-based summary recommendations, patient management tools or protocols). We developed a three-tiered model, a checklist and a glossary of common terms, for more efficient future production of better quality, contextually-relevant, locally-implementable SA PHC CPGs. Tier 1 involves transparent synthesis of existing high quality CPG recommendations; Tier 2 reflects local expertise to layer Tier 1 evidence with local contexts; and Tier 3 comprises tailored locally-relevant end-user guidance.
Our model could be relevant for any resource-poor environment. It should reduce effort and costs in finding and synthesising available research evidence, whilst efficiently focusing scant resources on contextually-relevant evidence-based guidance, and implementation.
国际公认的发展标准是高质量的全新临床实践指南(CPG)的基础。然而,对于高质量 CPG 应该“什么样”以及一个国家的高质量 CPG 是否可以在其他地方可行地实施,没有国际共识。编写全新的 CPG 通常需要大量的资源和资金,这在资源匮乏的环境中是具有挑战性的。本文提出了一种在这种情况下生成高质量 CPG 的替代、高效方法,即利用现有 CPG 并分层加入当地知识、背景和成果。
我们在南非(SA)初级卫生保健(PHC)中进行了一项混合方法的案例研究,该研究建立在四项独立研究的基础上。这些研究包括国际 CPG 活动概述、国际 CPG 开发实践的快速文献综述、对 16 个有针对性抽样的南非 PHC CPG 的严格评估,以及对这些 CPG 进行额外的询问,了解它们是如何、为何以及为谁编写的,以及它们的“外观”。
尽管目标是改善南非 PHC 的医疗保健实践,但纳入的 CPG 具有不同的、不明确的和不一致的制作过程、术语和证据呈现风格。没有一个与国际质量标准相符。然而,许多 CPG 包含了针对最终用户的创新简洁指导(我们将其归类为基于证据的总结建议、患者管理工具或方案)。我们开发了一个三层模型、一个检查表和一个常见术语词汇表,以更高效地制作更好质量、更具相关性、更能在当地实施的南非 PHC CPG。第 1 层涉及对现有高质量 CPG 建议进行透明的综合;第 2 层反映了当地的专业知识,将第 1 层证据与当地背景分层;第 3 层包括定制的当地相关最终用户指导。
我们的模型可能与任何资源匮乏的环境相关。它应该减少寻找和综合现有研究证据的努力和成本,同时有效地将稀缺资源集中在基于证据的相关指导和实施上。