Inserm U1132, Rheumatology Department, Lariboisière Hospital, Paris Diderot University, 2 rue Ambroise Paré, 75010, Paris, France.
Soladis Clinical Studies, Roubaix, France.
Arthritis Res Ther. 2018 May 2;20(1):78. doi: 10.1186/s13075-018-1585-0.
The uric acid (UA) level in patients with gout is a key factor in disease management and is typically measured in the laboratory using plasma samples obtained after venous puncture. This study aimed to assess the reliability of immediate UA measurement with capillary blood samples obtained by fingertip puncture with the HumaSens point-of-care meter.
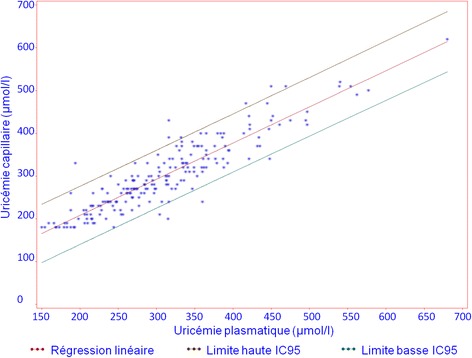
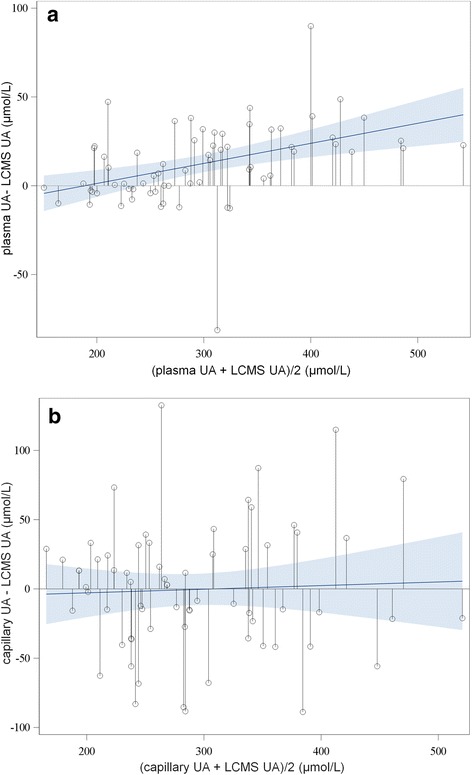
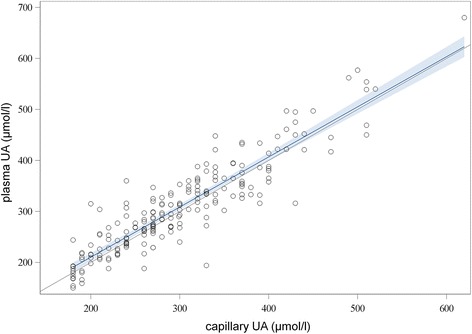
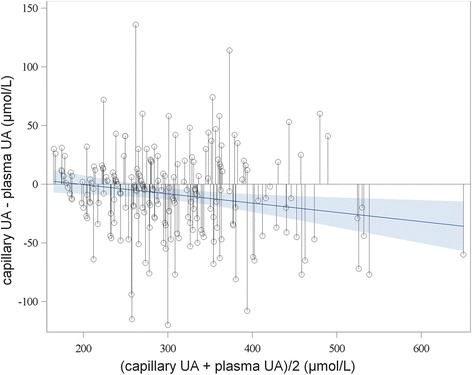
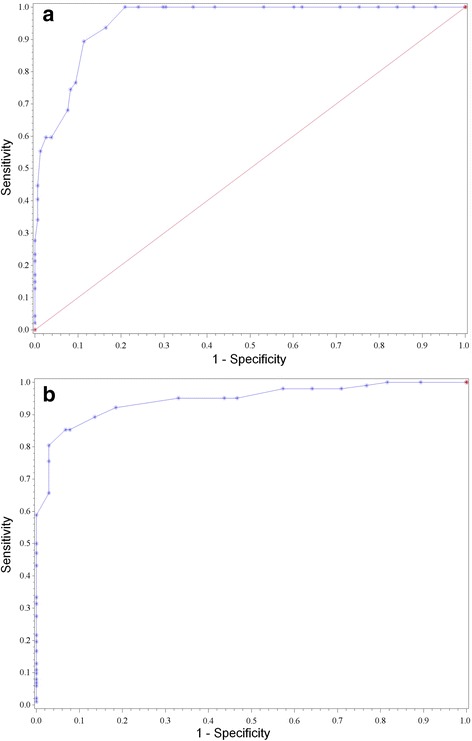
UA levels were measured using both the HumaSens meter in the clinic and the routine plasma UA method in the biochemistry laboratory of 238 consenting diabetic patients. HumaSens capillary and routine plasma UA measurements were compared by linear regression, Bland-Altman plots, intraclass correlation coefficient (ICC), and Lin's concordance coefficient. Values outside the dynamic range of the meter, low (LO) or high (HI), were analyzed separately. The best capillary UA thresholds for detecting hyperuricemia were determined by receiver operating characteristic (ROC) curves. The impact of potential confounding factors (demographic and biological parameters/treatments) was assessed. Capillary and routine plasma UA levels were compared to reference plasma UA measurements by liquid chromatography-mass spectrometry (LC-MS) for a subgroup of 67 patients.
In total, 205 patients had capillary and routine plasma UA measurements available. ICC was 0.90 (95% confidence interval (CI) 0.87-0.92), Lin's coefficient was 0.91 (0.88-0.93), and the Bland-Altman plot showed good agreement over all tested values. Overall, 17 patients showed values outside the dynamic range. LO values were concordant with plasma values, but HI values were considered uninterpretable. Capillary UA thresholds of 299 and 340 μmol/l gave the best results for detecting hyperuricemia (corresponding to routine plasma UA thresholds of 300 and 360 μmol/l, respectively). No significant confounding factor was found among those tested, except for hematocrit; however, this had a negligible influence on the assay reliability. When capillary and routine plasma results were discordant, comparison with LC-MS measurements showed that plasma measurements had better concordance: capillary UA, ICC 0.84 (95% CI 0.75-0.90), Lin's coefficient 0.84 (0.77-0.91); plasma UA, ICC 0.96 (0.94-0.98), Lin's coefficient 0.96 (0.94-0.98).
UA measurements with the HumaSens meter were reasonably comparable with those of the laboratory assay. The meter is easy to use and may be useful in the clinic and in epidemiologic studies.
痛风患者的尿酸(UA)水平是疾病管理的关键因素,通常在实验室使用静脉穿刺获得的血浆样本进行测量。本研究旨在评估使用指尖穿刺获得的毛细血管血样用 HumaSens 即时检测(POC)仪进行即时 UA 测量的可靠性。
对 238 名同意参与的糖尿病患者,使用 HumaSens 仪在诊所和生化实验室同时测量 UA 水平。采用线性回归、Bland-Altman 图、组内相关系数(ICC)和 Lin 一致性系数比较 HumaSens 毛细血管和常规血浆 UA 测量值。对超出仪器动态范围的低值(LO)或高值(HI)分别进行分析。通过受试者工作特征(ROC)曲线确定用于检测高尿酸血症的最佳毛细血管 UA 阈值。评估潜在混杂因素(人口统计学和生物学参数/治疗)的影响。对 67 名患者的亚组进行液相色谱-质谱(LC-MS)检测,比较毛细血管和常规血浆 UA 水平与参考血浆 UA 测量值。
共有 205 名患者有毛细血管和常规血浆 UA 测量值。ICC 为 0.90(95%置信区间(CI)0.87-0.92),Lin 系数为 0.91(0.88-0.93),Bland-Altman 图显示所有测试值均具有良好的一致性。总体上,有 17 名患者的测量值超出了动态范围。LO 值与血浆值一致,但 HI 值被认为无法解释。毛细血管 UA 阈值为 299 和 340 μmol/L 时,检测高尿酸血症的效果最佳(分别对应常规血浆 UA 阈值为 300 和 360 μmol/L)。除了红细胞压积外,未发现测试中的显著混杂因素,但对检测可靠性影响很小。当毛细血管和常规血浆结果不一致时,与 LC-MS 测量值比较显示,血浆测量值具有更好的一致性:毛细血管 UA,ICC 为 0.84(95% CI 0.75-0.90),Lin 系数为 0.84(0.77-0.91);血浆 UA,ICC 为 0.96(95% CI 0.94-0.98),Lin 系数为 0.96(95% CI 0.94-0.98)。
使用 HumaSens 仪进行 UA 测量与实验室检测具有较好的可比性。该仪器易于使用,可能在临床和流行病学研究中具有应用价值。