Institute of Development Studies, University of Dar es Salaam, P.O.BOX 35169, Dar es Salaam, Tanzania.
Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania.
Int J Equity Health. 2018 Oct 5;17(1):118. doi: 10.1186/s12939-018-0835-8.
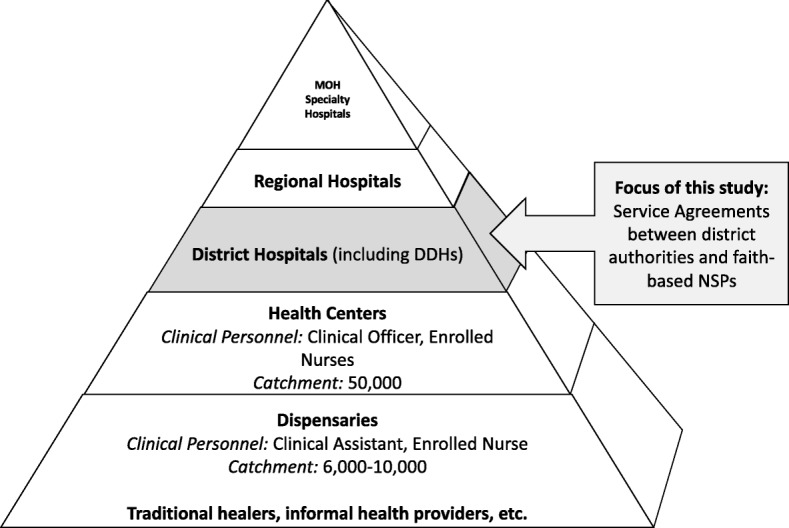
Governments increasingly recognize the need to engage non-state providers (NSPs) in health systems in order to move successfully towards Universal Health Coverage (UHC). One common approach to engaging NSPs is to contract-out the delivery of primary health care services. Research on contracting arrangements has typically focused on their impact on health service delivery; less is known about the actual processes underlying the development and implementation of interventions and the contextual factors that influence these. This paper reports on the design and implementation of service agreements (SAs) between local governments and NSPs for the provision of primary health care services in Tanzania. It examines the actors, policy process, context and policy content that influenced how the SAs were designed and implemented.
We used qualitative analytical methods to study the Tanzanian experience with contracting- out. Data were drawn from document reviews and in-depth interviews with 39 key informants, including six interviews at the national and regional levels and 33 interviews at the district level. All interviews were audiotaped, transcribed and translated into English. Data were managed in NVivo (version 10.0) and analyzed thematically.
The institutional frameworks shaping the engagement of the government with NSPs are rooted in Tanzania's long history of public-private partnerships in the health sector. Demand for contractual arrangements emerged from both the government and the faith-based organizations that manage NSP facilities. Development partners provided significant technical and financial support, signaling their approval of the approach. Although districts gained the mandate and power to make contractual agreements with NSPs, financing the contracts remained largely dependent on donor funds via central government budget support. Delays in reimbursements, limited financial and technical capacity of local government authorities and lack of trust between the government and private partners affected the implementation of the contractual arrangements.
Tanzania's central government needs to further develop the technical and financial capacity necessary to better support districts in establishing and financing contractual agreements with NSPs for primary health care services. Furthermore, forums for continuous dialogue between the government and contracted NSPs should be fostered in order to clarify the expectations of all parties and resolve any misunderstandings.
政府越来越认识到需要让非国家提供者(NSP)参与卫生系统,以便成功迈向全民健康覆盖(UHC)。让 NSP 参与的一种常见方法是将初级卫生保健服务进行外包。关于承包安排的研究通常侧重于其对卫生服务提供的影响;而对于干预措施背后的实际发展和实施过程以及影响这些过程的背景因素知之甚少。本文报告了坦桑尼亚地方政府与 NSP 之间为提供初级卫生保健服务而制定的服务协议(SA)的设计和实施情况。它研究了影响 SA 设计和实施的行为者、政策过程、背景和政策内容。
我们使用定性分析方法研究了坦桑尼亚的外包经验。数据来自文件审查和对 39 名主要知情人的深入访谈,其中包括在国家和区域一级的六次访谈和在地区一级的 33 次访谈。所有访谈均进行了录音、转录并翻译成英文。数据在 NVivo(版本 10.0)中进行管理,并进行了主题分析。
政府与 NSP 合作的制度框架根植于坦桑尼亚在卫生部门开展公私伙伴关系的悠久历史。对契约安排的需求既来自政府,也来自管理 NSP 设施的宗教组织。发展伙伴提供了大量的技术和财政支持,表明他们对这种方法的认可。尽管地区获得了与 NSP 签订合同的授权和权力,但合同的融资仍主要依赖中央政府预算支持的捐助资金。报销延迟、地方政府当局财政和技术能力有限以及政府与私人合作伙伴之间缺乏信任,影响了契约安排的实施。
坦桑尼亚中央政府需要进一步发展必要的技术和财政能力,以更好地支持地区与 NSP 就初级卫生保健服务建立和融资合同。此外,应促进政府与签约 NSP 之间的持续对话论坛,以澄清各方的期望并解决任何误解。