Nutrition and Clinical Services Division, International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Dhaka, Bangladesh.
Special Programme for Research and Training in Tropical Diseases (TDR), World Health Organization, Geneva, Switzerland.
Am J Trop Med Hyg. 2019 Jan;100(1):97-107. doi: 10.4269/ajtmh.18-0290.
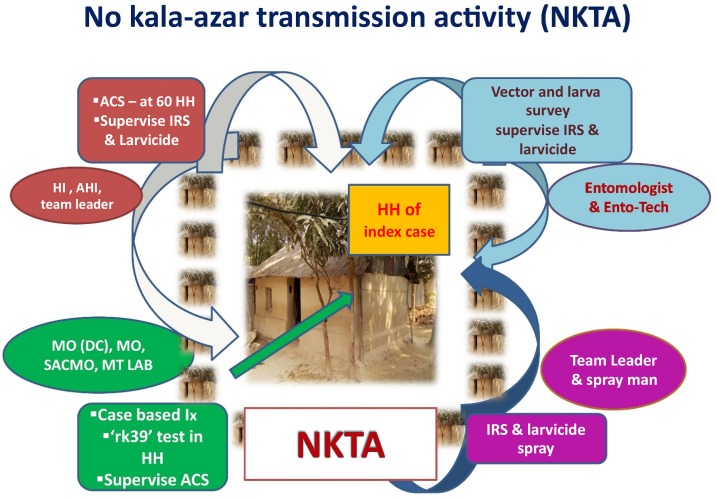
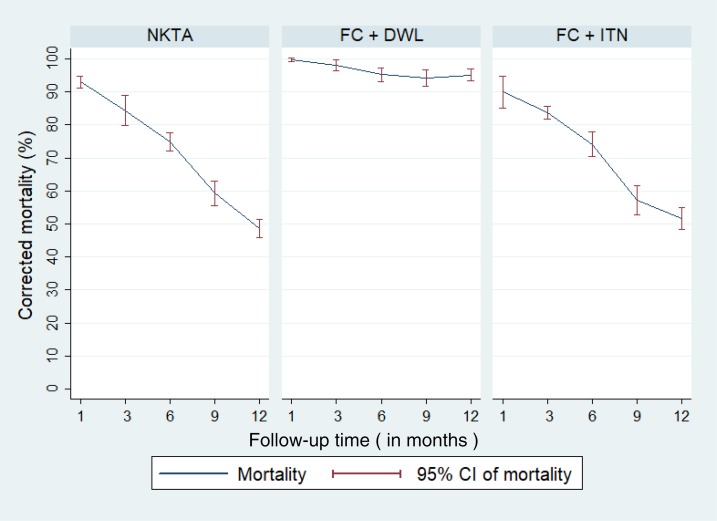
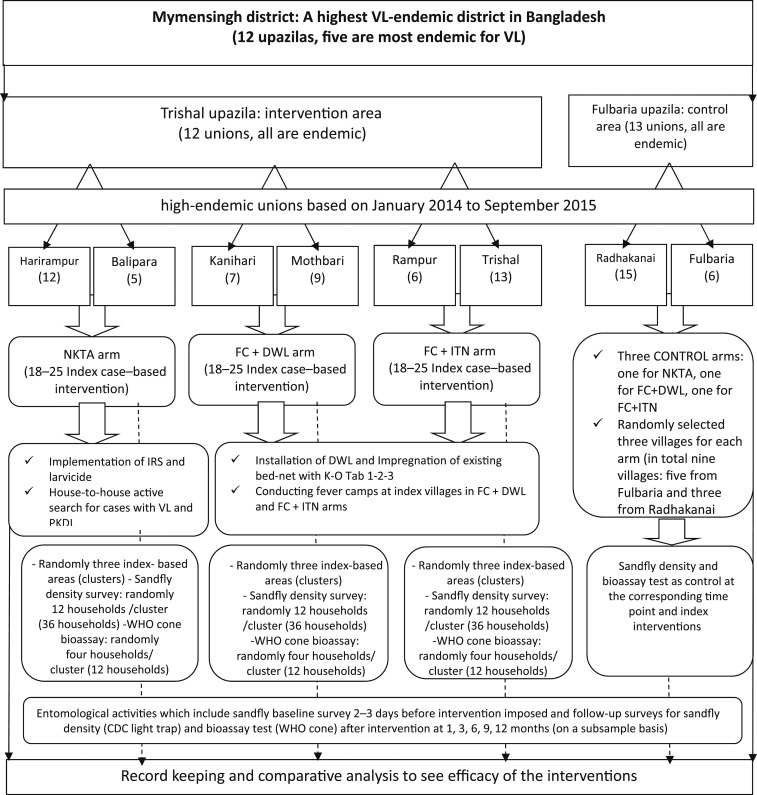
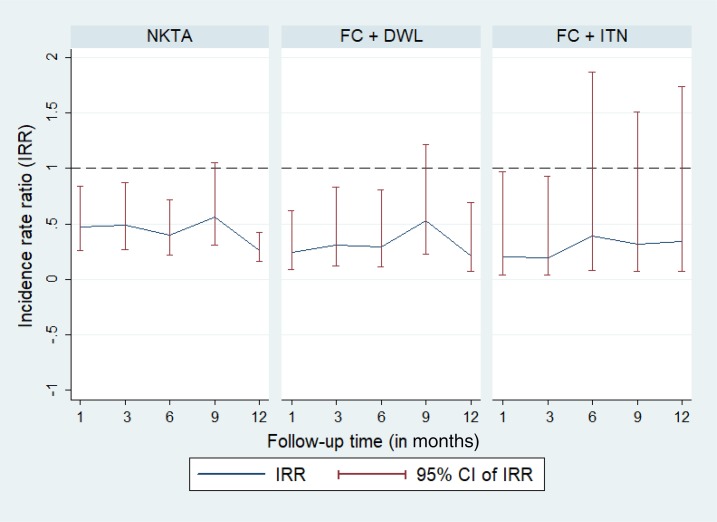
We compared the efficacy of three intervention packages for active case detection (ACD) of visceral leishmaniasis (VL)/post-kala-azar dermal leishmaniasis (PKDL) combined with sandfly control around an index case. The packages were 1) no kala-azar transmission activity involving indoor residual spraying (IRS) with deltamethrin, peri-domestic deployment of larvicide with temephos, and house-to-house search for cases; 2) fever camp (FC) plus durable wall lining (DWL) with deltamethrin; and 3) FC plus insecticide (deltamethrin) impregnated bed-nets (ITN) around an index case. Fever camp includes 1-day campaign at the village level to screen and diagnose VL, PKDL, leprosy, malaria, and tuberculosis among residents with chronic fever or skin disease. Efficacy was measured through yield of new cases, vector density reduction, and mortality at 1, 3, 6, 9, and 12 months following intervention. Fever camp + DWL was the most efficacious intervention package with 0.5 case detected per intervention, 79% reduction in vector density (incidence rate ratio [IRR] = 0.21, = 0.010), and 95.1% (95% confidence interval: 93.4%, 96.8%) sandfly mortality at 12 months. No kala-azar transmission activity was efficacious for vector control (74% vector reduction, IRR = 0.26, < 0.0001 at 9 months; and 84% sandfly mortality at 3 months), but not for case detection (0 case per intervention). Fever camp + ITN was efficacious in detection of VL/PKDL cases (0.43 case per intervention), but its efficacy for vector control was inconsistent. We recommend index case-based FC for ACD combined with DWL or IRS plus larvicide for sandfly control during the consolidation and maintenance phases of the VL elimination program of the Indian subcontinent.
我们比较了三种主动病例检测(ACD)方案干预包的疗效,这些方案用于检测内脏利什曼病(VL)/黑热病后皮肤利什曼病(PKDL),并结合按蚊控制,干预对象是一个索引病例周围的环境。这些方案包括:1)无黑热病传播活动,包括使用氯菊酯进行室内滞留喷洒(IRS)、在家庭周围使用敌百虫进行幼虫防治、以及挨家挨户搜索病例;2)发热营地(FC)加长效壁衬(DWL),使用氯菊酯;3)FC 加索引病例周围的驱虫(氯菊酯)浸渍蚊帐(ITN)。发热营地包括在村庄一级开展为期 1 天的活动,以筛查和诊断居民中的 VL、PKDL、麻风病、疟疾和结核病,对象为有慢性发热或皮肤病的居民。疗效通过新发病例的检出率、媒介密度降低率以及干预后 1、3、6、9 和 12 个月的死亡率来衡量。发热营地+DWL 是最有效的干预方案,每干预 1 例检出 0.5 例病例,媒介密度降低 79%(发病率比[IRR] = 0.21, = 0.010),12 个月时按蚊死亡率为 95.1%(95%置信区间:93.4%,96.8%)。无黑热病传播活动对控制媒介有效(9 个月时媒介减少 74%,IRR = 0.26, < 0.0001;3 个月时按蚊死亡率 84%),但对病例检出无效(每干预 0 例)。发热营地+ITN 对 VL/PKDL 病例的检出有效(每干预 0.43 例),但对媒介控制的效果不一致。我们建议在印度次大陆的 VL 消除计划的巩固和维持阶段,以基于索引病例的 FC 进行 ACD,结合 DWL 或 IRS 加幼虫防治来控制按蚊。