Drexel University College of Medicine, Philadelphia, PA, USA.
School of Medicine, University of California Irvine, Irvine, CA, USA.
Neuroimage Clin. 2019;21:101574. doi: 10.1016/j.nicl.2018.10.012. Epub 2018 Oct 14.
Imaging techniques used to measure hippocampal atrophy are key to understanding the clinical progression of Alzheimer's disease (AD). Various semi-automated hippocampal segmentation techniques are available and require human expert input to learn how to accurately segment new data. Our goal was to compare 1) the performance of our automated hippocampal segmentation technique relative to manual segmentations, and 2) the performance of our automated technique when provided with a training set from two different raters. We also explored the ability of hippocampal volumes obtained using manual and automated hippocampal segmentations to predict conversion from MCI to AD.
We analyzed 161 1.5 T T1-weighted brain magnetic resonance images (MRI) from the ADCS Donepezil/Vitamin E clinical study. All subjects carried a diagnosis of mild cognitive impairment (MCI). Three different segmentation outputs (one produced by manual tracing and two produced by a semi-automated algorithm trained with training sets developed by two raters) were compared using single measure intraclass correlation statistics (smICC). The radial distance method was used to assess each segmentation technique's ability to detect hippocampal atrophy in 3D. We then compared how well each segmentation method detected baseline hippocampal differences between MCI subjects who remained stable (MCInc) and those who converted to AD (MCIc) during the trial. Our statistical maps were corrected for multiple comparisons using permutation-based statistics with a threshold of p < .01.
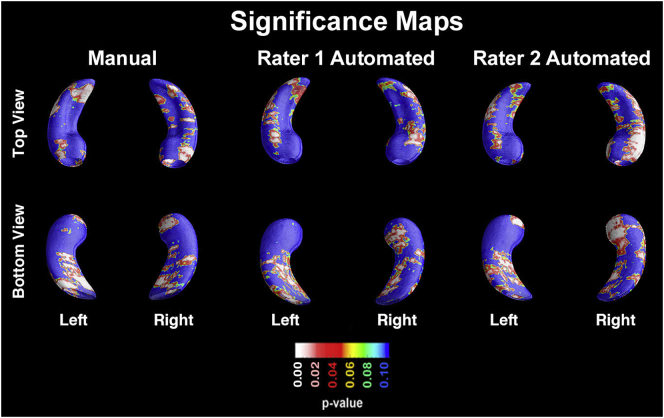
Our smICC analyses showed significant agreement between the manual and automated hippocampal segmentations from rater 1 [right smICC = 0.78 (95%CI 0.72-0.84); left smICC = 0.79 (95%CI 0.72-0.85)], the manual segmentations from rater 1 versus the automated segmentations from rater 2 [right smICC = 0.78 (95%CI 0.7-0.84); left smICC = 0.78 (95%CI 0.71-0.84)], and the automated segmentations of rater 1 versus rater 2 [right smICC = 0.97 (95%CI 0.96-0.98); left smICC = 0.97 (95%CI 0.96-0.98)]. All three segmentation methods detected significant CA1 and subicular atrophy in MCIc compared to MCInc at baseline (manual: right p = 0.0112, left p = 0.0006; automated rater 1: right p = 0.0318, left p = 0.0302; automated rater 2: right p = 0.0029, left p = 0.0166).
The hippocampal volumes obtained with a fast semi-automated segmentation method were highly comparable to the ones obtained with the labor-intensive manual segmentation method. The AdaBoost automated hippocampal segmentation technique is highly reliable allowing the efficient analysis of large data sets.
用于测量海马体萎缩的成像技术是理解阿尔茨海默病(AD)临床进展的关键。有各种半自动海马体分割技术,需要人类专家的输入来学习如何准确地分割新数据。我们的目标是比较 1)我们的自动海马体分割技术相对于手动分割的性能,以及 2)当提供来自两个不同评分者的训练集时,我们的自动技术的性能。我们还探讨了使用手动和自动海马体分割获得的海马体体积来预测从 MCI 到 AD 的转化的能力。
我们分析了来自 ADCS 多奈哌齐/维生素 E 临床研究的 161 个 1.5T T1 加权脑磁共振图像(MRI)。所有受试者均诊断为轻度认知障碍(MCI)。使用单测量组内相关统计(smICC)比较了三种不同的分割输出(一种由手动跟踪产生,两种由由两位评分者开发的训练集训练的半自动算法产生)。使用放射状距离法评估每种分割技术在 3D 中检测海马体萎缩的能力。然后,我们比较了每种分割方法在试验期间在基线时如何检测到保持稳定的 MCI 受试者(MCInc)和转化为 AD 的 MCI 受试者(MCIc)之间的海马体差异。我们的统计地图使用基于置换的统计数据进行了多重比较校正,阈值为 p<0.01。
我们的 smICC 分析显示,评分者 1 的手动和自动海马体分割之间存在显著的一致性[右侧 smICC=0.78(95%CI 0.72-0.84);左侧 smICC=0.79(95%CI 0.72-0.85)],评分者 1 的手动分割与评分者 2 的自动分割之间存在显著一致性[右侧 smICC=0.78(95%CI 0.7-0.84);左侧 smICC=0.78(95%CI 0.71-0.84)],以及评分者 1 的自动分割与评分者 2 的自动分割之间存在显著一致性[右侧 smICC=0.97(95%CI 0.96-0.98);左侧 smICC=0.97(95%CI 0.96-0.98)]。与 MCInc 相比,所有三种分割方法均在基线时检测到 MCIc 的 CA1 和亚皮质萎缩(手动:右侧 p=0.0112,左侧 p=0.0006;自动评分者 1:右侧 p=0.0318,左侧 p=0.0302;自动评分者 2:右侧 p=0.0029,左侧 p=0.0166)。
使用快速半自动分割方法获得的海马体体积与使用劳动密集型手动分割方法获得的体积高度可比。AdaBoost 自动海马体分割技术非常可靠,允许对大型数据集进行高效分析。