Pisani Elizabeth, Nistor Adina-Loredana, Hasnida Amalia, Parmaksiz Koray, Xu Jingying, Kok Maarten Oliver
Policy Institute, King's College London, London, London, WC2B 6LE, UK.
Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, London, WC1E 7HT, UK.
Wellcome Open Res. 2019 Apr 16;4:70. doi: 10.12688/wellcomeopenres.15236.1. eCollection 2019.
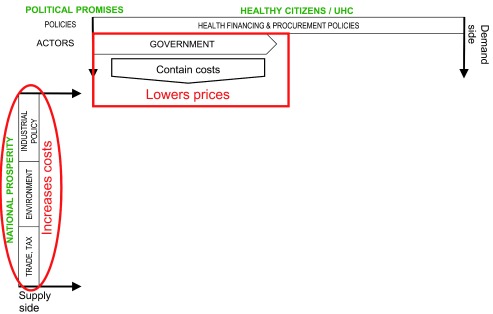
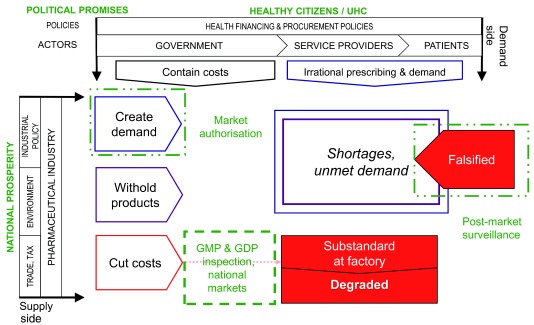
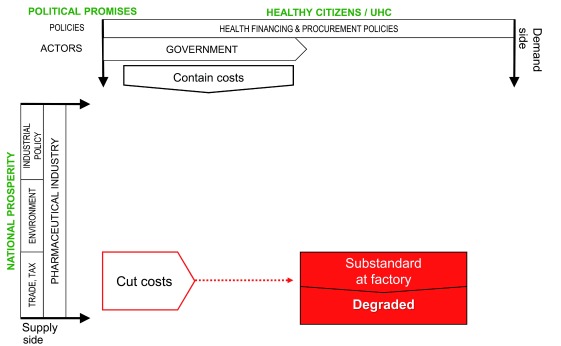
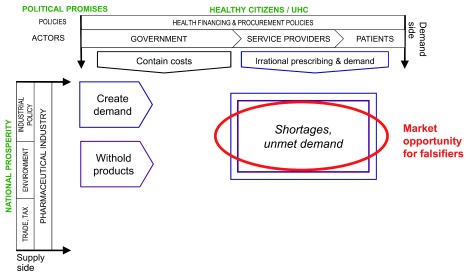
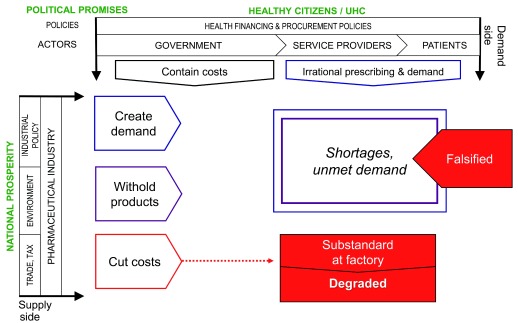
Substandard and falsified medicines undermine health systems. We sought to unravel the political and economic factors which drive the production of these products, and to explain how they reach patients. We conducted in-depth case studies in China, Indonesia, Turkey and Romania. We reviewed academic papers and press reports (n = 840), developing semi-structured questionnaires. We interviewed regulators, policy-makers, pharmaceutical manufacturers, physicians, pharmacists, patients and academics (n=88). We coded data using NVivo software, and developed an analytic framework to assess national risks for substandard and falsified medicines. We tested the framework against cases reported to the World Health Organization, from countries at all income levels. We found that increasing political commitment to provision of universal health coverage has led to public procurement policies aimed at lowering prices of medical products. In response, legitimate, profit-driven pharmaceutical companies protect their margins by cutting costs, or withdrawing from less profitable markets, while distributors engage in arbitrage. Meanwhile, health providers sometimes protect profits by 'upselling' patients to medicines not covered by insurers. Cost-cutting can undermine quality assurance, leading to substandard or degraded medicines. Other responses contribute to shortages, irrational demand and high prices. All of these provide market opportunities for producers of falsified products; they also push consumers outside of the regular supply chain, providing falsifiers with easy access to customers. The analytic framework capturing these interactions explained cases in most high and middle-income settings; additional factors operate in the poorest countries. Most efforts to secure medicine quality currently focus on product regulation. However, our research suggests market mechanisms are key drivers for poor quality medicines, including where political commitments to universal health coverage are under-resourced. We have developed a framework to guide country-specific, system-wide analysis. This can flag risks and pinpoint specific actions to protect medicine quality, and thus health.
不合格药品和假药损害卫生系统。我们试图剖析推动这些产品生产的政治和经济因素,并解释它们是如何到达患者手中的。我们在中国、印度尼西亚、土耳其和罗马尼亚开展了深入的案例研究。我们查阅了学术论文和新闻报道(共840篇),并编制了半结构化问卷。我们采访了监管机构人员、政策制定者、制药商、医生、药剂师、患者和学者(共88人)。我们使用NVivo软件对数据进行编码,并建立了一个分析框架来评估不合格药品和假药的国家风险。我们根据向世界卫生组织报告的来自所有收入水平国家的案例对该框架进行了测试。我们发现,各国在提供全民健康覆盖方面的政治承诺不断增强,导致出台了旨在降低医疗产品价格的公共采购政策。对此,合法的、以盈利为导向的制药公司通过削减成本或退出利润较低的市场来保护自身利润空间,而经销商则进行套利活动。与此同时,医疗服务提供者有时会通过向患者“推销”保险公司不承保的药品来保护利润。削减成本可能会破坏质量保证,导致药品不合格或质量下降。其他应对措施则造成药品短缺、不合理需求和高价。所有这些都为假药生产者提供了市场机会;它们还将消费者推向常规供应链之外,使造假者能够轻易接触到客户。这个捕捉到这些相互作用的分析框架解释了大多数高收入和中等收入环境下的案例;在最贫穷国家还有其他因素在起作用。目前,确保药品质量的大多数努力都集中在产品监管上。然而,我们的研究表明,市场机制是劣质药品的关键驱动因素,包括在对全民健康覆盖的政治承诺资金不足的情况下。我们已经建立了一个框架来指导针对具体国家的全系统分析。这可以标记风险并确定保护药品质量从而保障健康的具体行动。