China Center for Health Development Studies, Peking University, Beijing, China.
School of Management, Beijing University of Chinese Medicine, Beijing, China.
PLoS One. 2020 Jan 21;15(1):e0227956. doi: 10.1371/journal.pone.0227956. eCollection 2020.
We aimed to analyze regional disparities of health care resources in traditional Chinese medicine (TCM) county hospitals and their time trends, and to assess the changes of regional disparities before and after 2009 health care reforms.
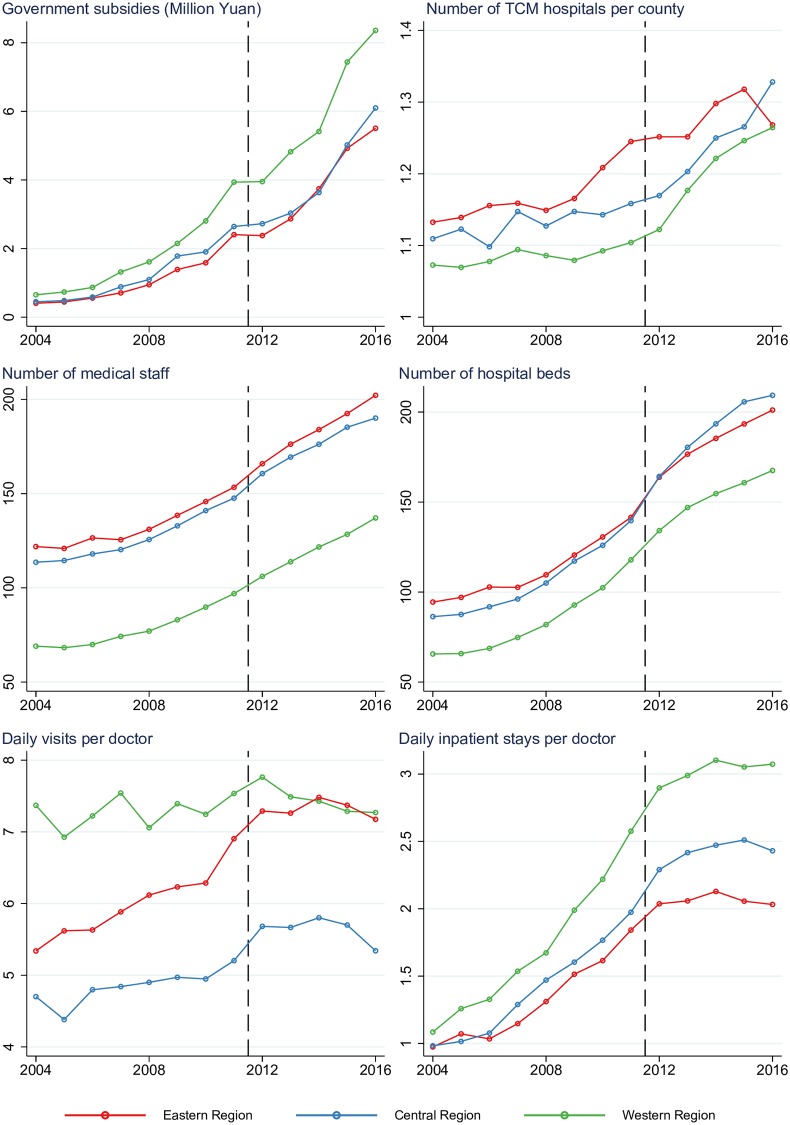
We used hospital-based, longitudinal data from all TCM county hospitals in China between 2004 and 2016. To measure the key development features of TCM county hospitals, data were collected on government hospital investment, hospital numbers (the average number of TCM hospitals per county), hospital scale (the number of medical staff and hospital beds) and doctors' workload (the daily visits and inpatient stays per doctor). We used segmented linear regression to test the time trend for outcome variables. We set a breakpoint at 2011, dividing the pre-reform (2004-2011) and post-reform (2012-2016) periods.
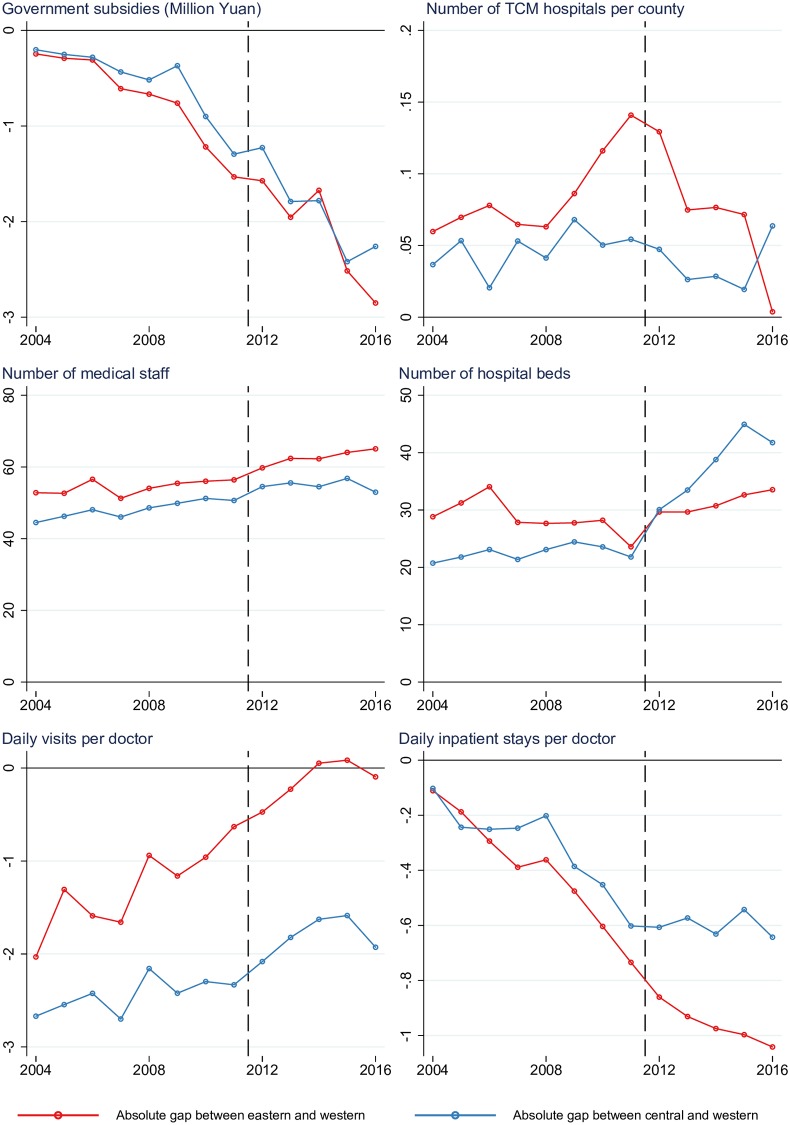
After the 2009 health reforms, TCM hospitals continued to display large disparities in the number, scale, and doctors' workload across the three regions. In the pre-reform period, yearly government subsidies for TCM hospitals in western area were roughly RMB0.6 million (US$89 thousand) more than those in central and eastern region, which increased under the 2009 reforms to roughly RMB2 million (US$298 thousand) more per yer in post-reform period. These increased subsidies saw an increase in the number of TCM hospitals in the western area, partly addressing regional disparities. But there was no improvement in the regional disparities in terms of scale (number of beds) and the doctors' workload (daily outpatient visits and inpatients per doctor) increased or remained unchanged between the western and other regions.
Although TCM hospital number, scale, and doctors' workload increased over the past 13 years, substantial regional disparities remained. The 2009 health reforms did not significantly change the regional disparities in health care resources, especially between the eastern and western regions.
分析中医县级医院卫生资源的区域差异及其时间趋势,并评估医改前后(2009 年)区域差异的变化。
我们使用了 2004 年至 2016 年期间中国所有中医县级医院的基于医院的纵向数据。为了衡量中医县级医院的关键发展特征,我们收集了政府对医院的投资、医院数量(每个县平均中医院数量)、医院规模(医务人员和病床数量)以及医生工作量(每位医生的日门诊和住院人数)的数据。我们使用分段线性回归来检验结果变量的时间趋势。我们在 2011 年设置了一个断点,将医改前(2004-2011 年)和医改后(2012-2016 年)两个时期分开。
医改后,中医医院在三个地区的数量、规模和医生工作量方面仍然存在较大差异。在医改前,西部地区中医医院每年获得的政府补贴比中部和东部地区多约 600 万元人民币(89 万美元),医改后这一数字增加到每年约 2000 万元人民币(298 万美元)。这些增加的补贴使得西部地区中医医院的数量有所增加,部分缓解了区域差异。但是,在规模(床位数)和医生工作量(每位医生的日门诊和住院人数)方面,区域差异并没有改善,西部地区与其他地区之间的差距仍然存在。
尽管中医医院的数量、规模和医生工作量在过去 13 年中有所增加,但仍然存在显著的区域差异。2009 年的医改并没有显著改变卫生资源的区域差异,尤其是在东部和西部地区之间。