Jain Nickul Saral, Nguyen Ailene, Formanek Blake, Alluri Ram, Buser Zorica, Hah Ray, Wang Jeffrey Chun
Department of Orthopaedic Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
Asian Spine J. 2020 Oct;14(5):647-654. doi: 10.31616/asj.2019.0246. Epub 2020 Mar 30.
Retrospective review of insurance database.
To investigate national trends, complications, and costs after cervical disc replacement (CDR) using an administrative insurance database representative of the United States population.
As CDR continues to be used to treat patients with cervical stenosis, it is important to gain a better understanding of its use on a national level, potential complications, and cost. This information will allow for optimal patient counseling, risk stratification, and healthcare cost assessments. Several prior studies have investigated complications associated with CDR, but they have been limited by small sample size, single institution experiences, limited follow-up, and potential conflicts of interest.
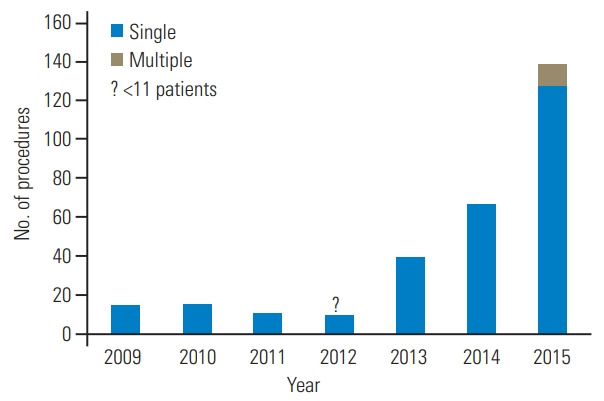
Patients who underwent single or multilevel CDR between 2007 and 2015 were identified using an insurance database. We collected data on annual trends, reimbursement costs, patient demographic information, hospital information, and information on complications from the time of operation to 1 year postoperative.
Total of 293 patients underwent either single or multilevel CDR. The number of procedures increased nonlinearly over time at an average of 17% per year, with a greater increase seen in the outpatient setting. Less than 3.7% of patients had new onset pain within 1 year after CDR. Within 1 year, 12.3% of patients reported a mechanical and/or bone-related complication. There were no patients who indicated a new nerve injury within 6 months of follow-up. Less than 3.7% of patients presented with dysphagia or dysphonia within 6 months, infection within 3 months, or a revision or reoperation within 1 year. Average reimbursement for single-level inpatient versus outpatient CDR was US $33,696.28 and US $34,675.12, respectively (p=0.29).
This study demonstrated that the use of CDR continued to increase. The most common complication was mechanical and/or bone-related, and cost analysis demonstrated no significant difference between inpatient and outpatient CDR.
对保险数据库进行回顾性分析。
利用一个代表美国人口的行政保险数据库,调查颈椎间盘置换术(CDR)后的全国趋势、并发症及费用情况。
随着CDR持续用于治疗颈椎管狭窄患者,在国家层面更好地了解其应用情况、潜在并发症及费用非常重要。这些信息将有助于进行最佳的患者咨询、风险分层及医疗费用评估。此前有多项研究调查了与CDR相关的并发症,但这些研究存在样本量小、单机构经验、随访有限以及潜在利益冲突等局限性。
利用保险数据库识别出2007年至2015年间接受单节段或多节段CDR的患者。我们收集了年度趋势、报销费用、患者人口统计学信息、医院信息以及从手术时到术后1年的并发症信息。
共有293例患者接受了单节段或多节段CDR。手术例数随时间呈非线性增加,平均每年增加17%,门诊手术的增幅更大。CDR术后1年内,不到3.7%的患者出现新发疼痛。1年内,12.3%的患者报告出现机械性和/或与骨相关的并发症。随访6个月内,没有患者出现新的神经损伤。不到3.7%的患者在6个月内出现吞咽困难或发音障碍,3个月内出现感染,或1年内需要翻修或再次手术。单节段住院和门诊CDR的平均报销费用分别为33,696.28美元和34,675.12美元(p = 0.29)。
本研究表明CDR的应用持续增加。最常见的并发症是机械性和/或与骨相关的并发症,费用分析显示住院和门诊CDR之间无显著差异。