Xu Yuejia, Wood Angela M, Sweeting Michael J, Roberts David J, Tom Brian Dm
MRC Biostatistics Unit, University of Cambridge, Cambridge, UK.
Cardiovascular Epidemiology Unit, University of Cambridge, Cambridge, UK.
Stat Methods Med Res. 2020 Nov;29(11):3113-3134. doi: 10.1177/0962280220920669. Epub 2020 May 8.
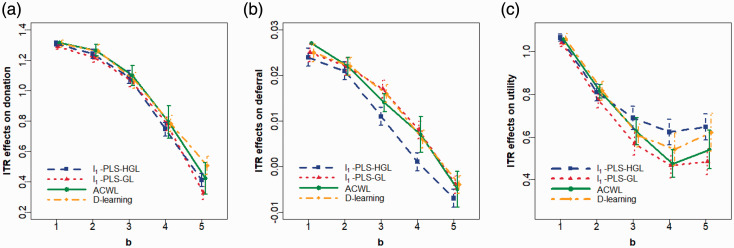
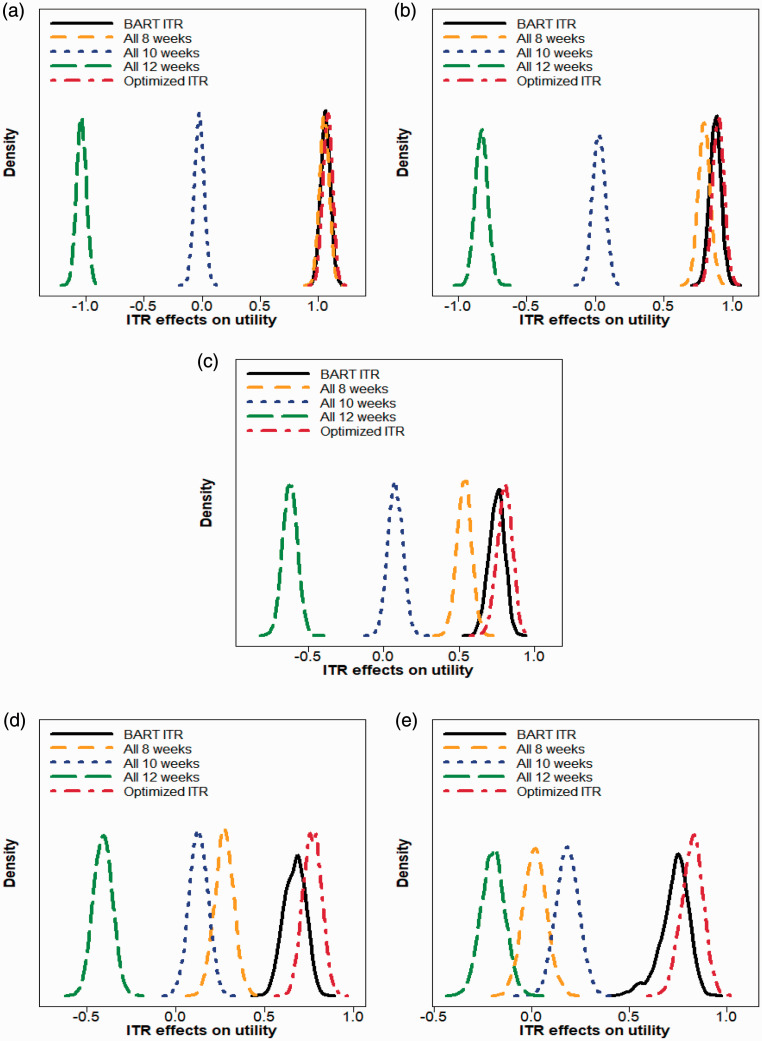
There is a growing interest in precision medicine where individual heterogeneity is incorporated into decision-making and treatments are tailored to individuals to provide better healthcare. One important aspect of precision medicine is the estimation of the optimal individualized treatment rule (ITR) that optimizes the expected outcome. Most methods developed for this purpose are restricted to the setting with two treatments, while clinical studies with more than two treatments are common in practice. In this work, we summarize methods to estimate the optimal ITR in the multi-arm setting and compare their performance in large-scale clinical trials via simulation studies. We then illustrate their utilities with a case study using the data from the INTERVAL trial, which randomly assigned over 20,000 male blood donors from England to one of the three inter-donation intervals (12-week, 10-week, and eight-week) over two years. We estimate the optimal individualized donation strategies under three different objectives. Our findings are fairly consistent across five different approaches that are applied: when we target the maximization of the total units of blood collected, almost all donors are assigned to the eight-week inter-donation interval, whereas if we aim at minimizing the low hemoglobin deferral rates, almost all donors are assigned to donate every 12 weeks. However, when the goal is to maximize the utility score that "discounts" the total units of blood collected by the incidences of low hemoglobin deferrals, we observe some heterogeneity in the optimal inter-donation interval across donors and the optimal donor assignment strategy is highly dependent on the trade-off parameter in the utility function.
精准医学越来越受到关注,在精准医学中,个体异质性被纳入决策过程,治疗方案根据个体情况量身定制,以提供更好的医疗保健。精准医学的一个重要方面是估计优化预期结果的最佳个体化治疗规则(ITR)。为此目的开发的大多数方法仅限于两种治疗的情况,而在实际临床研究中,有两种以上治疗的情况很常见。在这项工作中,我们总结了在多臂设置中估计最佳ITR的方法,并通过模拟研究比较了它们在大规模临床试验中的性能。然后,我们通过一个案例研究来说明它们的效用,该案例研究使用了INTERVAL试验的数据,该试验在两年内将来自英格兰的20000多名男性献血者随机分配到三个不同的献血间隔(12周、10周和8周)之一。我们在三个不同目标下估计最佳个体化献血策略。我们的发现对于应用的五种不同方法来说相当一致:当我们以采集的血液总量最大化为目标时,几乎所有献血者都被分配到8周的献血间隔,而如果我们旨在最小化低血红蛋白延期率,几乎所有献血者都被分配为每12周献血一次。然而,当目标是最大化通过低血红蛋白延期发生率“折扣”采集的血液总量的效用分数时,我们观察到不同献血者的最佳献血间隔存在一些异质性,并且最佳献血者分配策略高度依赖于效用函数中的权衡参数。