Rundo Leonardo, Beer Lucian, Ursprung Stephan, Martin-Gonzalez Paula, Markowetz Florian, Brenton James D, Crispin-Ortuzar Mireia, Sala Evis, Woitek Ramona
Department of Radiology, University of Cambridge, Cambridge CB2 0QQ, UK; Cancer Research UK Cambridge Centre, University of Cambridge, Cambridge CB2 0RE, UK.
Department of Radiology, University of Cambridge, Cambridge CB2 0QQ, UK; Cancer Research UK Cambridge Centre, University of Cambridge, Cambridge CB2 0RE, UK; Department of Biomedical Imaging and Image-guided Therapy, Medical University Vienna, Vienna 1090, Austria.
Comput Biol Med. 2020 May;120:103751. doi: 10.1016/j.compbiomed.2020.103751. Epub 2020 Apr 10.
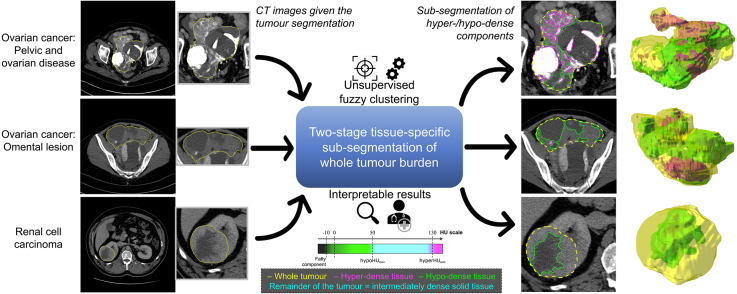
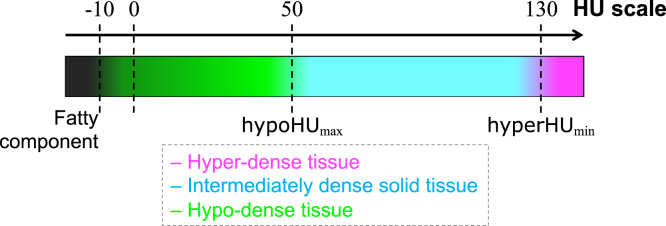
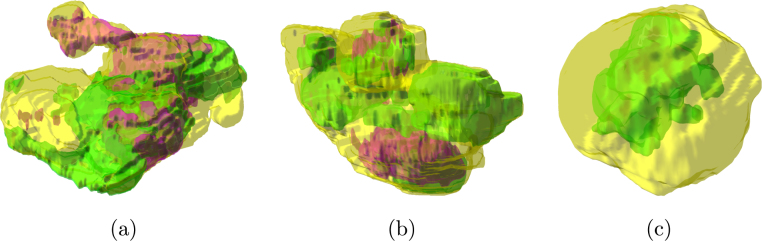
Cancer typically exhibits genotypic and phenotypic heterogeneity, which can have prognostic significance and influence therapy response. Computed Tomography (CT)-based radiomic approaches calculate quantitative features of tumour heterogeneity at a mesoscopic level, regardless of macroscopic areas of hypo-dense (i.e., cystic/necrotic), hyper-dense (i.e., calcified), or intermediately dense (i.e., soft tissue) portions.
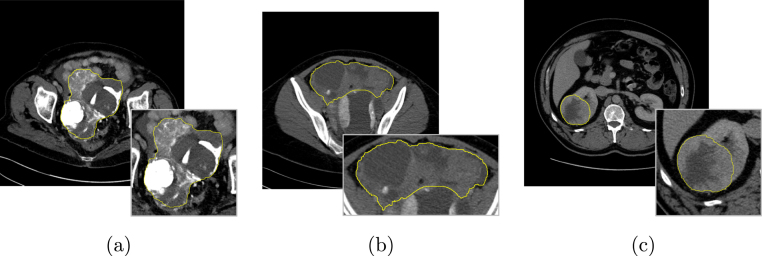
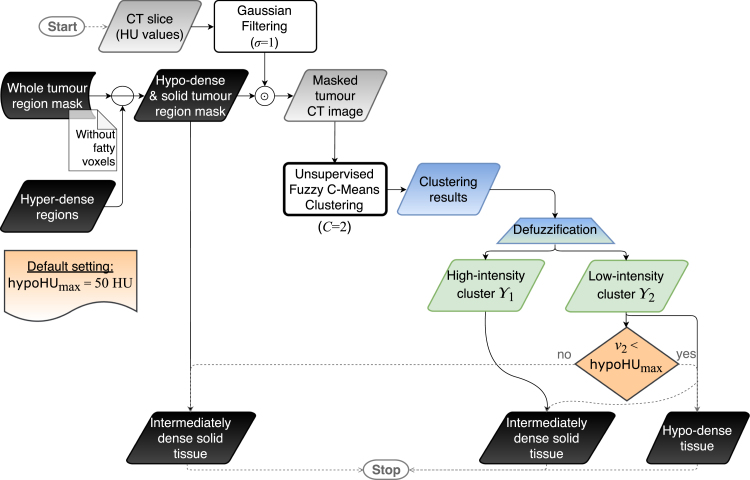
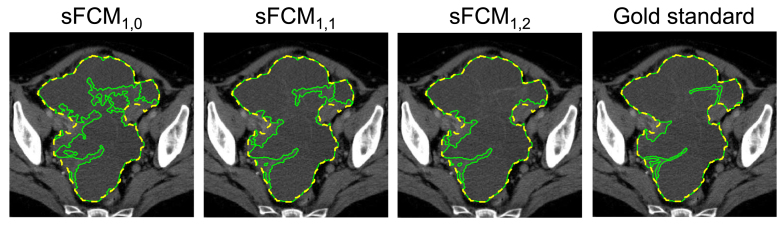
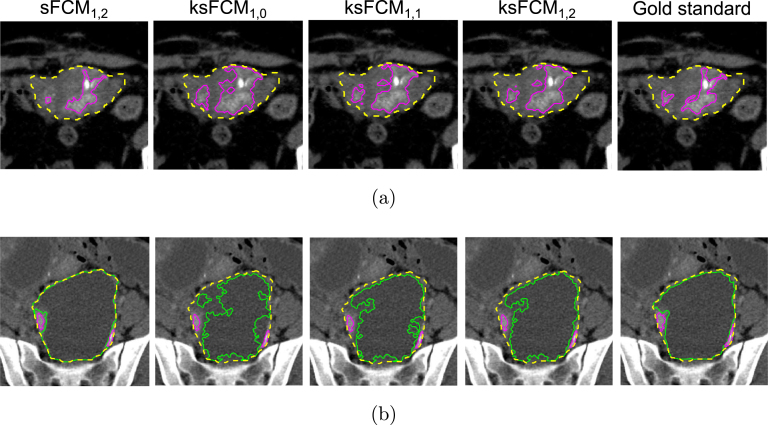
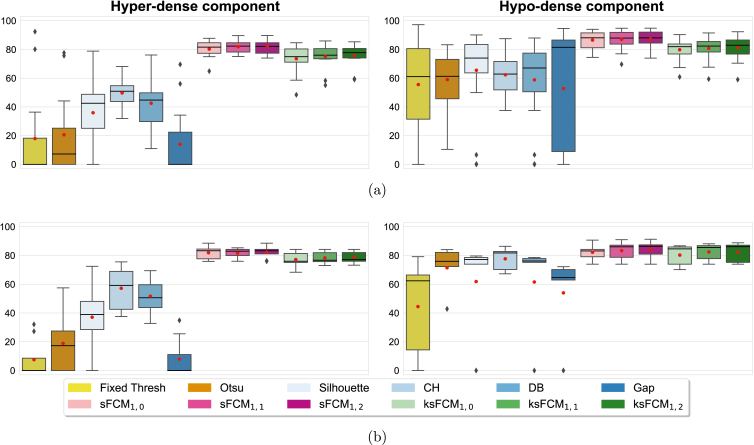
With the goal of achieving the automated sub-segmentation of these three tissue types, we present here a two-stage computational framework based on unsupervised Fuzzy C-Means Clustering (FCM) techniques. No existing approach has specifically addressed this task so far. Our tissue-specific image sub-segmentation was tested on ovarian cancer (pelvic/ovarian and omental disease) and renal cell carcinoma CT datasets using both overlap-based and distance-based metrics for evaluation.
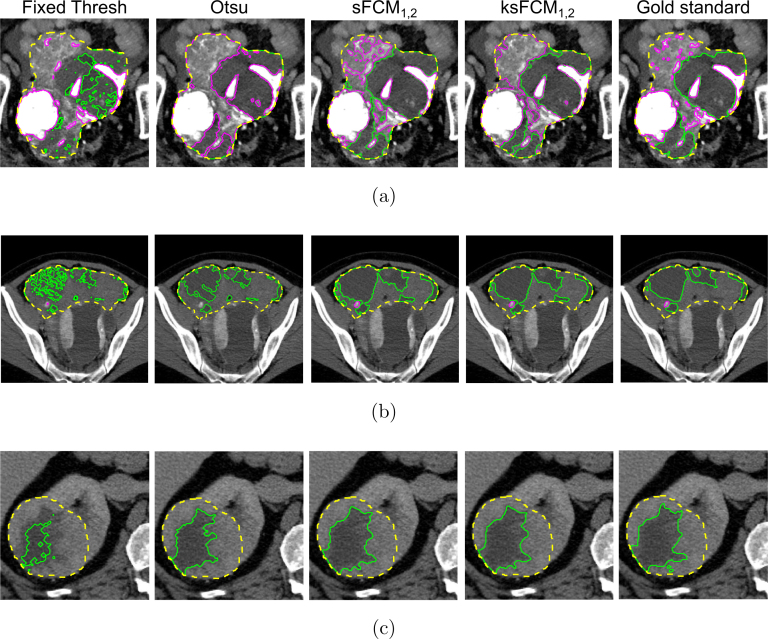
On all tested sub-segmentation tasks, our two-stage segmentation approach outperformed conventional segmentation techniques: fixed multi-thresholding, the Otsu method, and automatic cluster number selection heuristics for the K-means clustering algorithm. In addition, experiments showed that the integration of the spatial information into the FCM algorithm generally achieves more accurate segmentation results, whilst the kernelised FCM versions are not beneficial. The best spatial FCM configuration achieved average Dice similarity coefficient values starting from 81.94±4.76 and 83.43±3.81 for hyper-dense and hypo-dense components, respectively, for the investigated sub-segmentation tasks.
The proposed intelligent framework could be readily integrated into clinical research environments and provides robust tools for future radiomic biomarker validation.
癌症通常表现出基因和表型异质性,这可能具有预后意义并影响治疗反应。基于计算机断层扫描(CT)的放射组学方法可在介观水平计算肿瘤异质性的定量特征,而无需考虑低密度(即囊性/坏死性)、高密度(即钙化)或中等密度(即软组织)部分的宏观区域。
为了实现这三种组织类型的自动子分割,我们在此提出一种基于无监督模糊C均值聚类(FCM)技术的两阶段计算框架。到目前为止,尚无现有方法专门解决此任务。我们的组织特异性图像子分割在卵巢癌(盆腔/卵巢和网膜疾病)和肾细胞癌CT数据集上进行了测试,使用基于重叠和基于距离的指标进行评估。
在所有测试的子分割任务中,我们的两阶段分割方法优于传统分割技术:固定多阈值分割、大津法以及K均值聚类算法的自动聚类数选择启发式方法。此外,实验表明,将空间信息集成到FCM算法中通常可获得更准确的分割结果,而核化的FCM版本并无益处。对于所研究的子分割任务,最佳空间FCM配置分别为高密度和低密度成分实现的平均骰子相似系数值,起始值分别为81.94±4.76和83.43±3.81。
所提出的智能框架可轻松集成到临床研究环境中,并为未来放射组学生物标志物验证提供强大工具。