Fortius Clinic, London, UK.
Orthopaedic Surgery Department, Chelsea and Westminster Hospital, London, UK.
Knee Surg Sports Traumatol Arthrosc. 2020 Dec;28(12):3700-3708. doi: 10.1007/s00167-020-06084-4. Epub 2020 Jun 5.
The purpose of this study was to determine the contribution of each of the ACL and medial ligament structures in resisting anteromedial rotatory instability (AMRI) loads applied in vitro.
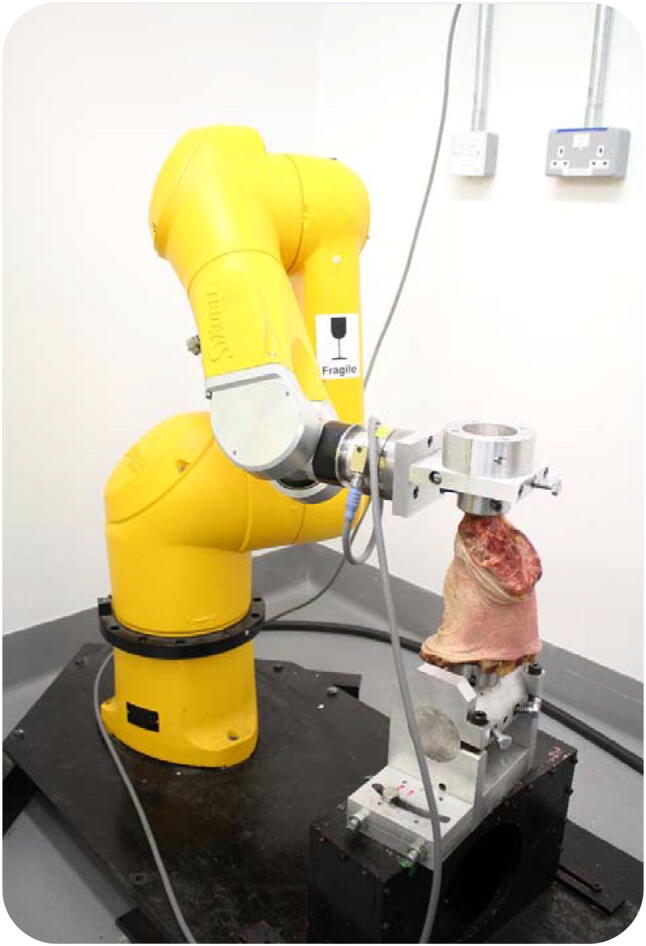
Twelve knees were tested using a robotic system. It imposed loads simulating clinical laxity tests at 0° to 90° flexion: ±90 N anterior-posterior force, ±8 Nm varus-valgus moment, and ±5 Nm internal-external rotation, and the tibial displacements were measured in the intact knee. The ACL and individual medial structures-retinaculum, superficial and deep medial collateral ligament (sMCL and dMCL), and posteromedial capsule with oblique ligament (POL + PMC)-were sectioned sequentially. The tibial displacements were reapplied after each cut and the reduced loads required allowed the contribution of each structure to be calculated.
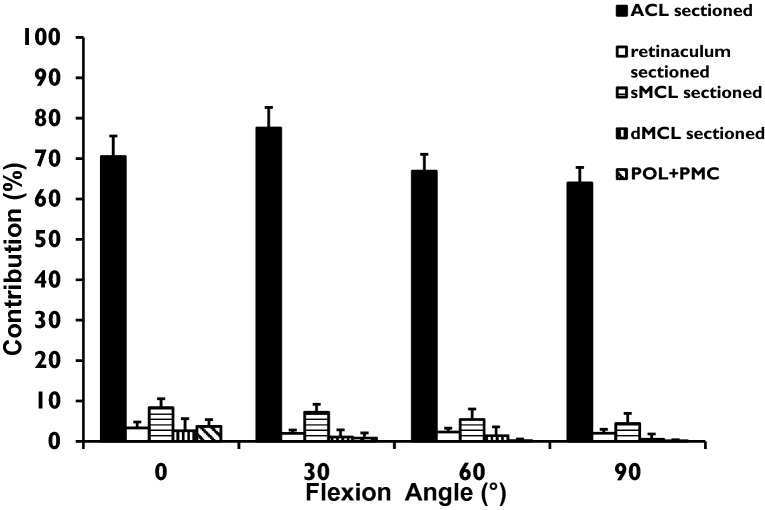
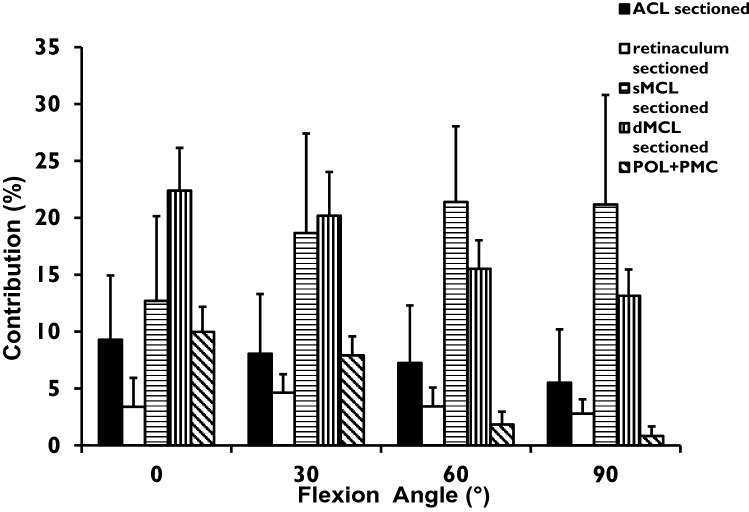
For anterior translation, the ACL was the primary restraint, resisting 63-77% of the drawer force across 0° to 90°, the sMCL contributing 4-7%. For posterior translation, the POL + PMC contributed 10% of the restraint in extension; other structures were not significant. For valgus load, the sMCL was the primary restraint (40-54%) across 0° to 90°, the dMCL 12%, and POL + PMC 16% in extension. For external rotation, the dMCL resisted 23-13% across 0° to 90°, the sMCL 13-22%, and the ACL 6-9%.
The dMCL is the largest medial restraint to tibial external rotation in extension. Therefore, following a combined ACL + MCL injury, AMRI may persist if there is inadequate healing of both the sMCL and dMCL, and MCL deficiency increases the risk of ACL graft failure.
本研究旨在确定 ACL 和内侧韧带结构在抵抗体外施加的前内侧旋转不稳定(AMRI)负荷中的各自贡献。
使用机器人系统对 12 个膝关节进行测试。它施加了模拟临床松弛测试的负荷,在 0°至 90°的屈曲范围内:±90 N 前后力、±8 Nm 内翻-外翻力矩和±5 Nm 内外旋转,并且在完整的膝关节中测量胫骨位移。ACL 和单独的内侧结构-支持带、浅层和深层内侧副韧带(sMCL 和 dMCL)以及后内侧囊伴斜韧带(POL + PMC)-被依次切断。在每次切割后重新施加胫骨位移,所需的减少负荷允许计算每个结构的贡献。
对于前向平移,ACL 是主要的限制因素,在 0°至 90°范围内抵抗 63-77%的抽屉力,sMCL 贡献 4-7%。对于后向平移,POL + PMC 在伸展时对 10%的限制有贡献;其他结构没有显著作用。对于外翻负荷,sMCL 在 0°至 90°范围内是主要的限制因素(40-54%),dMCL 为 12%,POL + PMC 在伸展时为 16%。对于外旋,dMCL 在 0°至 90°范围内抵抗 23-13%,sMCL 为 13-22%,ACL 为 6-9%。
在伸展时,dMCL 是最大的内侧限制胫骨外旋的因素。因此,如果 sMCL 和 dMCL 的愈合都不充分,ACL 和 MCL 损伤后可能会持续存在 AMRI,如果 MCL 缺失,ACL 移植物失败的风险会增加。