School of Computing, Queen's University, Kingston, K7L 3N6, Canada.
Department of Critical Care Medicine, Queen's University, Kingston, K7L 2V7, Canada.
Sci Rep. 2020 Jul 10;10(1):11480. doi: 10.1038/s41598-020-67952-0.
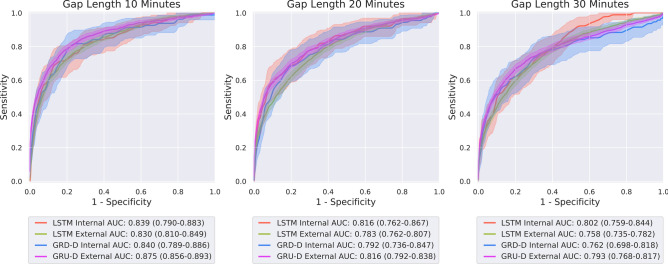
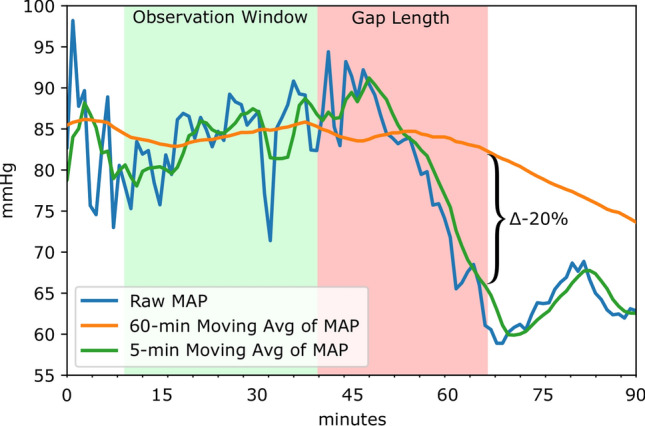
The vast quantities of data generated and collected in the Intensive Care Unit (ICU) have given rise to large retrospective datasets that are frequently used for observational studies. The temporal nature and fine granularity of much of the data collected in the ICU enable the pursuit of predictive modeling. In particular, forecasting acute hypotensive episodes (AHE) in intensive care patients has been of interest to researchers in critical care medicine. Given an advance warning of an AHE, care providers may be prompted to search for evolving disease processes and help mitigate negative clinical outcomes. However, the conventionally adopted definition of an AHE does not account for inter-patient variability and is restrictive. To reflect the wider trend of global clinical and research efforts in precision medicine, we introduce a patient-specific definition of AHE in this study and propose deep learning based models to predict this novel definition of AHE in data from multiple independent institutions. We provide extensive evaluation of the models by studying their accuracies in detecting patient-specific AHEs with lead-times ranging from 10 min to 1 hour before the onset of the event. The resulting models achieve AUROC values ranging from 0.57-0.87 depending on the lead time of the prediction. We demonstrate the generalizability and robustness of our approach through the use of independent multi-institutional data.
重症监护病房(ICU)中产生和收集的大量数据导致了大型回顾性数据集,这些数据集经常被用于观察性研究。ICU 中收集的许多数据具有时间性质和细粒度,这使得可以进行预测建模。特别是,预测重症监护患者的急性低血压发作(AHE)一直是重症监护医学研究人员感兴趣的问题。如果事先预警 AHE,护理人员可能会被提示寻找正在发展的疾病过程,并帮助减轻负面的临床结果。然而,传统上采用的 AHE 定义没有考虑到患者间的变异性,并且具有限制性。为了反映全球临床和研究在精准医学方面的广泛趋势,我们在本研究中引入了一种患者特异性的 AHE 定义,并提出了基于深度学习的模型,以预测来自多个独立机构的数据中的这种新的 AHE 定义。我们通过研究模型在检测从事件发生前 10 分钟到 1 小时不等的患者特异性 AHE 方面的准确性,对模型进行了广泛的评估。根据预测的提前时间,得到的模型的 AUROC 值范围为 0.57-0.87。我们通过使用独立的多机构数据证明了我们方法的通用性和鲁棒性。