Anantham Devanand, Chai-Lim Crystal, Zhou Jamie Xuelian, Phua Ghee Chee
Duke-NUS Medical School, Singapore, Singapore.
Department of Respiratory and Critical Care Medicine, Singapore General Hospital, Academia Building Level 3, 20 College Road, Singapore, S169856 Singapore.
J Intensive Care. 2020 Aug 6;8:59. doi: 10.1186/s40560-020-00475-y. eCollection 2020.
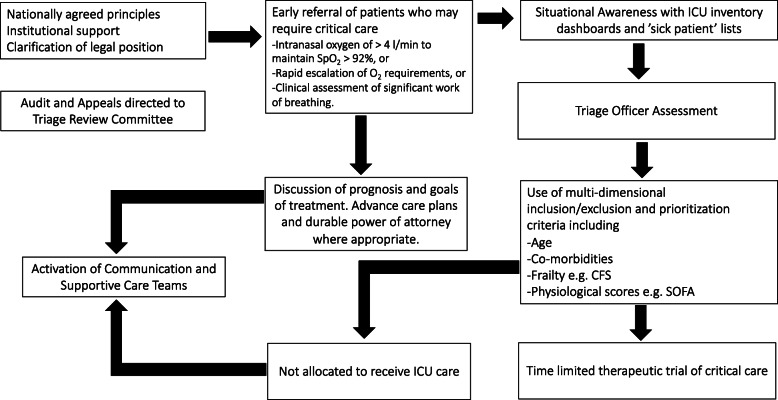
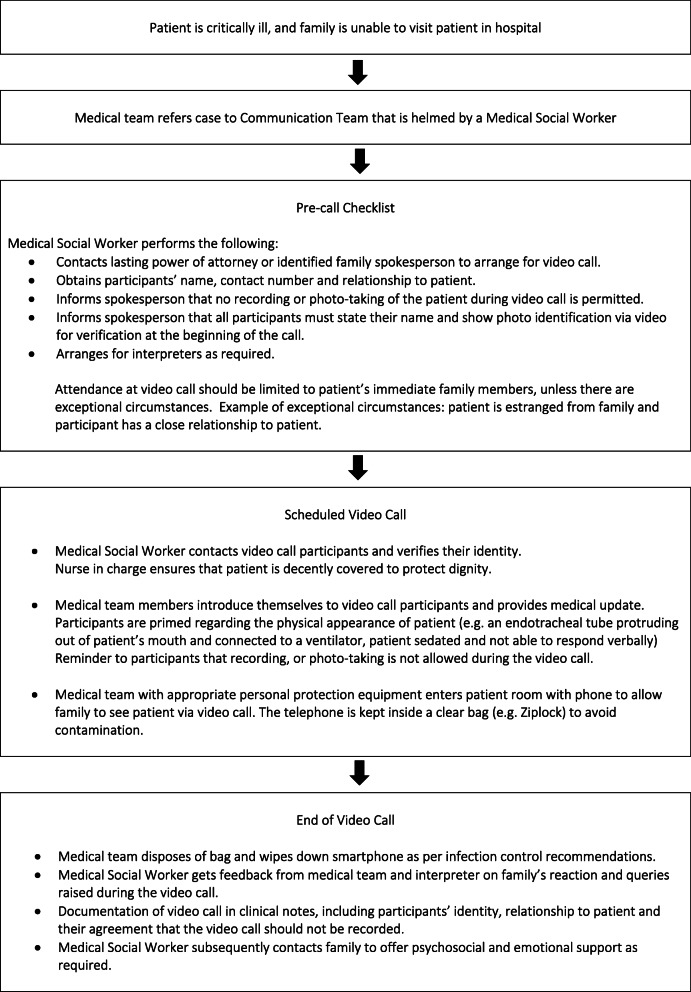
Triage becomes necessary when demand for intensive care unit (ICU) resources exceeds supply. Without triage, there is a risk that patients will be admitted to the ICU in the sequence that they present, disadvantaging those who either present later or have poorer access to healthcare. Moreover, if the patients with the best prognosis are not allocated life support, there is the possibility that overall mortality will increase. Before formulating criteria, principles such as maximizing lives saved and fairness ought to have been agreed upon to guide decision-making. The triage process is subdivided into three parts, i.e., having explicit inclusion/exclusion criteria for ICU admission, prioritization of patients for allocation to available beds, and periodic reassessment of all patients already admitted to the ICU. Multi-dimensional criteria offer more holistic prognostication than only using age cutoffs. Appointed triage officers should also be enabled to make data-driven decisions. However, the process does not merely end with an allocation decision being made. Any decision has to be sensitively and transparently communicated to the patient and family. With infection control measures, there are challenges in managing communication and the psychosocial distress of dying alone. Therefore, explicit video call protocols and social services expertise will be necessary to mitigate these challenges. Besides symptom management and psychosocial management, supportive care teams play an integral role in coordination of complex cases. This scoping review found support for the three-pronged, triage-communication-supportive care approach to facilitate the smooth operationalization of the triage process in a pandemic.
当重症监护病房(ICU)资源的需求超过供给时,分诊就变得必要。如果没有分诊,患者有可能按照就诊顺序被收入ICU,这对那些就诊较晚或获得医疗服务机会较差的患者不利。此外,如果没有将预后最佳的患者分配到生命支持资源,总体死亡率有可能会上升。在制定标准之前,应该先就诸如挽救更多生命和公平等原则达成共识,以指导决策。分诊过程分为三个部分,即制定明确的ICU收治纳入/排除标准、对患者进行优先级排序以分配到可用床位,以及对所有已收入ICU的患者进行定期重新评估。多维标准比分年龄段标准能提供更全面的预后评估。还应使指定的分诊人员能够做出基于数据的决策。然而,这个过程并不只是以做出分配决定而告终。任何决定都必须以敏感且透明的方式传达给患者及其家属。在采取感染控制措施的情况下,在管理沟通以及独自面对死亡所带来的心理社会痛苦方面存在挑战。因此,需要明确的视频通话协议和社会服务专业知识来应对这些挑战。除了症状管理和心理社会管理之外,支持性护理团队在协调复杂病例方面发挥着不可或缺的作用。这篇综述发现,三管齐下的分诊 - 沟通 - 支持性护理方法有助于在大流行期间使分诊过程顺利实施。