Pathology Department, VUMC, Amsterdam UMC, Amsterdam, the Netherlands.
Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, UK.
Clin Exp Immunol. 2020 Nov;202(2):193-209. doi: 10.1111/cei.13523. Epub 2020 Oct 12.
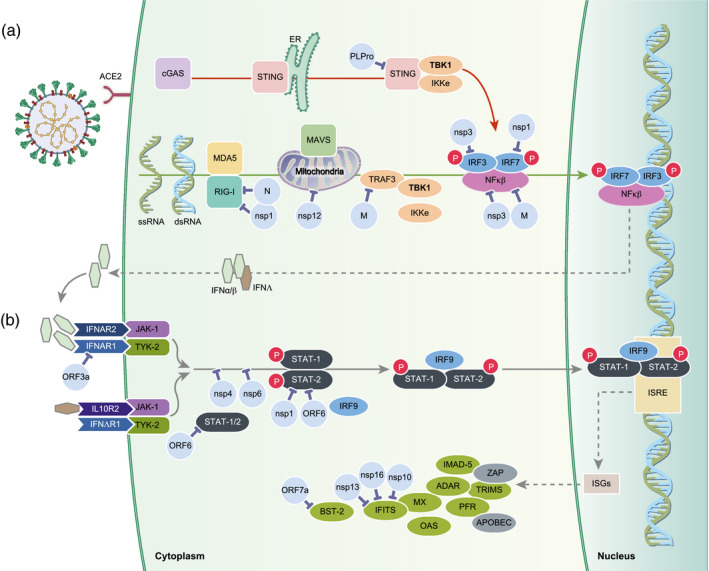
Innate immune sensing of viral molecular patterns is essential for development of antiviral responses. Like many viruses, SARS-CoV-2 has evolved strategies to circumvent innate immune detection, including low cytosine-phosphate-guanosine (CpG) levels in the genome, glycosylation to shield essential elements including the receptor-binding domain, RNA shielding and generation of viral proteins that actively impede anti-viral interferon responses. Together these strategies allow widespread infection and increased viral load. Despite the efforts of immune subversion, SARS-CoV-2 infection activates innate immune pathways inducing a robust type I/III interferon response, production of proinflammatory cytokines and recruitment of neutrophils and myeloid cells. This may induce hyperinflammation or, alternatively, effectively recruit adaptive immune responses that help clear the infection and prevent reinfection. The dysregulation of the renin-angiotensin system due to down-regulation of angiotensin-converting enzyme 2, the receptor for SARS-CoV-2, together with the activation of type I/III interferon response, and inflammasome response converge to promote free radical production and oxidative stress. This exacerbates tissue damage in the respiratory system, but also leads to widespread activation of coagulation pathways leading to thrombosis. Here, we review the current knowledge of the role of the innate immune response following SARS-CoV-2 infection, much of which is based on the knowledge from SARS-CoV and other coronaviruses. Understanding how the virus subverts the initial immune response and how an aberrant innate immune response contributes to the respiratory and vascular damage in COVID-19 may help to explain factors that contribute to the variety of clinical manifestations and outcome of SARS-CoV-2 infection.
先天免疫感知病毒的分子模式对于抗病毒反应的发展至关重要。与许多病毒一样,SARS-CoV-2 已经进化出了规避先天免疫检测的策略,包括基因组中低胞嘧啶-磷酸-鸟嘌呤(CpG)水平、糖基化以保护包括受体结合域在内的必需元件、RNA 屏蔽以及生成积极阻碍抗病毒干扰素反应的病毒蛋白。这些策略共同导致广泛的感染和增加的病毒载量。尽管存在免疫颠覆的努力,SARS-CoV-2 感染仍会激活先天免疫途径,诱导强烈的 I/III 型干扰素反应、促炎细胞因子的产生以及中性粒细胞和髓样细胞的募集。这可能会引发过度炎症,或者有效地招募适应性免疫反应,帮助清除感染并防止再次感染。由于 SARS-CoV-2 的受体血管紧张素转换酶 2 的下调,肾素-血管紧张素系统的失调,加上 I/III 型干扰素反应和炎性小体反应的激活,共同促进自由基的产生和氧化应激。这会加剧呼吸系统的组织损伤,但也会导致广泛的凝血途径激活导致血栓形成。在这里,我们综述了 SARS-CoV-2 感染后先天免疫反应的作用的现有知识,其中大部分是基于对 SARS-CoV 和其他冠状病毒的了解。了解病毒如何颠覆初始免疫反应以及异常的先天免疫反应如何导致 COVID-19 中的呼吸道和血管损伤,可能有助于解释导致 SARS-CoV-2 感染临床表现和结果多样化的因素。