Department of Surgical Sciences, Department of Obstetrics and Gynaecology, University of Cagliari, SS 554 - bivio Sestu, Monserrato, 09032, Cagliari, Italy.
Queen Margaret University, Institute for Global Health and Development, Edinburgh, EH21 6UU, Scotland, UK.
BMC Pregnancy Childbirth. 2020 Dec 10;20(1):770. doi: 10.1186/s12884-020-03462-1.
Improvements in medical technologies have seen over-medicalization of childbirth. Caesarean section (CS) is a lifesaving procedure proven effective in reducing maternal and perinatal mortality across the globe. However, as with any medical procedure, the CS intrinsically carries some risk to its beneficiaries. In recent years, CS rates have risen alarmingly in high-income countries. Many exceeding the World Health Organisation (WHO) recommendation of a 10 to 15% annual CS rate. While this situation poses an increased risk to women and their children, it also represents an excess human and financial burden on health systems. Therefore, from a health system perspective this study systematically summarizes existing evidence relevant to the factors driving the phenomenon of increasing CS rates using Italy as a case study.
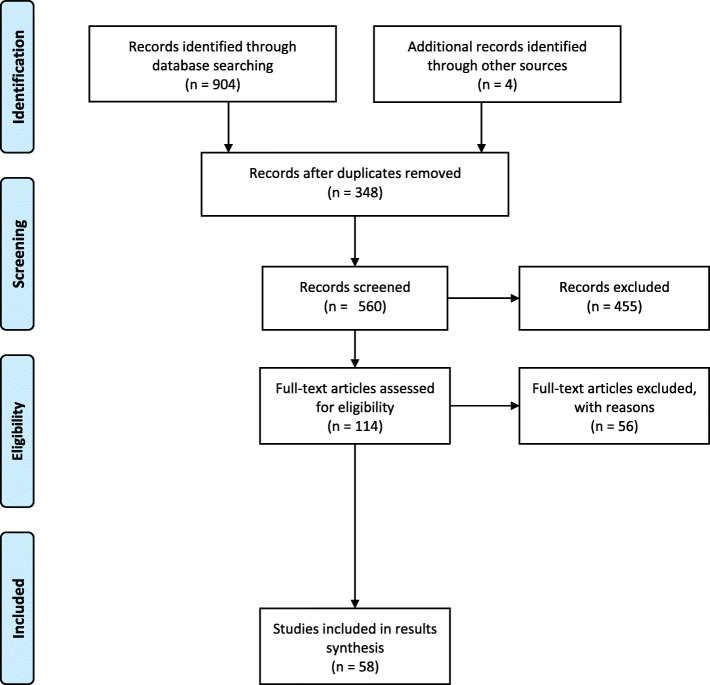
Employing the WHO Health System Framework (WHOHSF), this systematic review used the PRISMA guidelines to report findings. PubMed, SCOPUS, MEDLINE, Cochrane Library and Google Scholar databases were searched up until April 1, 2020. Findings were organised through the six dimensions of the WHOHSF framework: service delivery, health workforce, health system information; medical products vaccine and technologies, financing; and leadership and governance.
CS rates in Italy are affected by complex interactions among several stakeholder groups and contextual factors such as the hyper-medicalisation of delivery, differences in policy and practice across units and the national context, issues pertaining to the legal and social environment, and women's attitudes towards pregnancy and childbirth.
Mitigating the high rates of CS will require a synergistic multi-stakeholder intervention. Specifically, with processes able to attract the official endorsement of policy makers, encourage concensus between regional authorities and local governments and guide the systematic compliance of delivery units with its clinical guidelines.
医疗技术的进步导致了分娩的过度医疗化。剖宫产(CS)是一种已被证明在全球范围内有效降低孕产妇和围产期死亡率的救生程序。然而,与任何医疗程序一样,CS 本身对其受益者也存在一些风险。近年来,高收入国家的 CS 率惊人地上升。许多国家的 CS 率超过了世界卫生组织(WHO)建议的每年 10%至 15%的 CS 率。虽然这种情况对妇女及其子女构成了更大的风险,但也对卫生系统造成了额外的人力和财政负担。因此,从卫生系统的角度来看,本研究系统地总结了与导致 CS 率上升现象相关的现有证据,以意大利为例。
本系统评价采用世界卫生组织卫生系统框架(WHOHSF),并按照 PRISMA 指南报告研究结果。检索了 PubMed、SCOPUS、MEDLINE、Cochrane 图书馆和 Google Scholar 数据库,检索时间截至 2020 年 4 月 1 日。研究结果通过 WHOHSF 框架的六个维度进行组织:服务提供、卫生人力、卫生系统信息;医疗产品、疫苗和技术、筹资;以及领导力和治理。
意大利的 CS 率受到几个利益相关者群体和情境因素之间的复杂相互作用的影响,例如分娩的过度医疗化、单位之间政策和实践的差异、与法律和社会环境相关的问题,以及妇女对怀孕和分娩的态度。
降低 CS 的高比率需要多利益攸关方的协同干预。具体来说,需要能够吸引决策者正式支持的流程,鼓励区域当局和地方政府之间达成共识,并指导分娩单位系统地遵守其临床指南。