Department of Infectious Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
Centre for the Mathematical Modelling of Infectious Diseases, London School of Hygiene and Tropical Medicine, London, UK.
BMC Med. 2020 Dec 15;18(1):397. doi: 10.1186/s12916-020-01865-7.
Cholera epidemics continue to challenge disease control, particularly in fragile and conflict-affected states. Rapid detection and response to small cholera clusters is key for efficient control before an epidemic propagates. To understand the capacity for early response in fragile states, we investigated delays in outbreak detection, investigation, response, and laboratory confirmation, and we estimated epidemic sizes. We assessed predictors of delays, and annual changes in response time.
We compiled a list of cholera outbreaks in fragile and conflict-affected states from 2008 to 2019. We searched for peer-reviewed articles and epidemiological reports. We evaluated delays from the dates of symptom onset of the primary case, and the earliest dates of outbreak detection, investigation, response, and confirmation. Information on how the outbreak was alerted was summarized. A branching process model was used to estimate epidemic size at each delay. Regression models were used to investigate the association between predictors and delays to response.
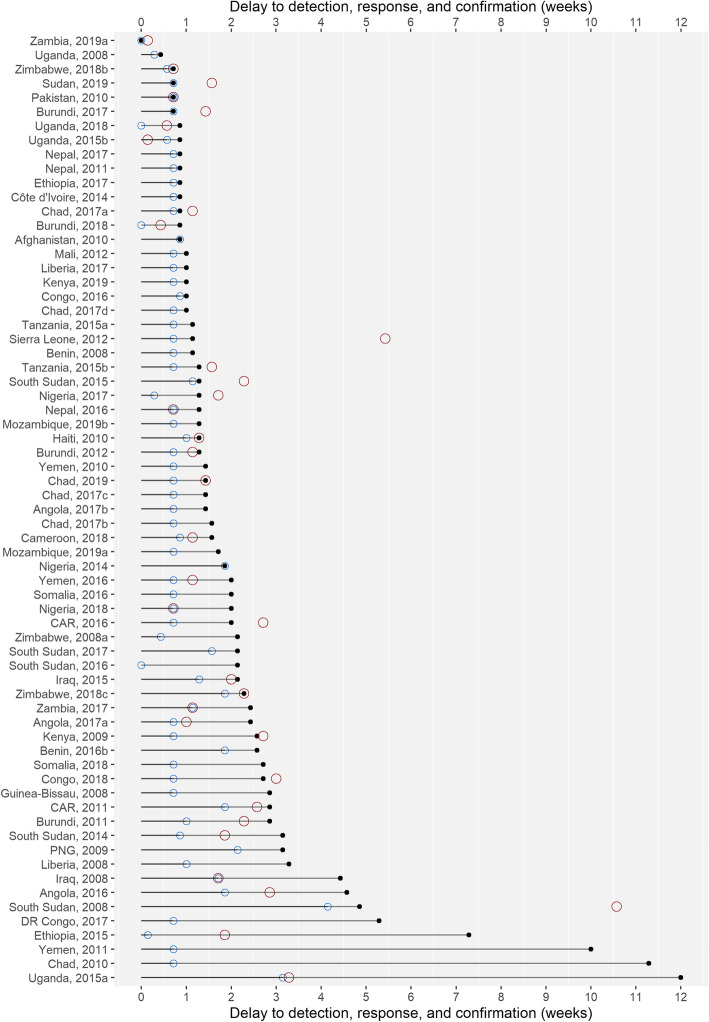
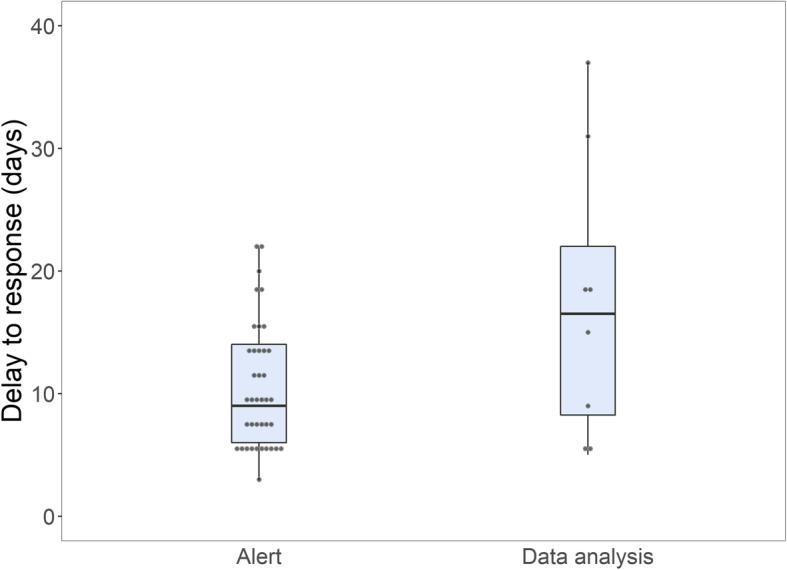
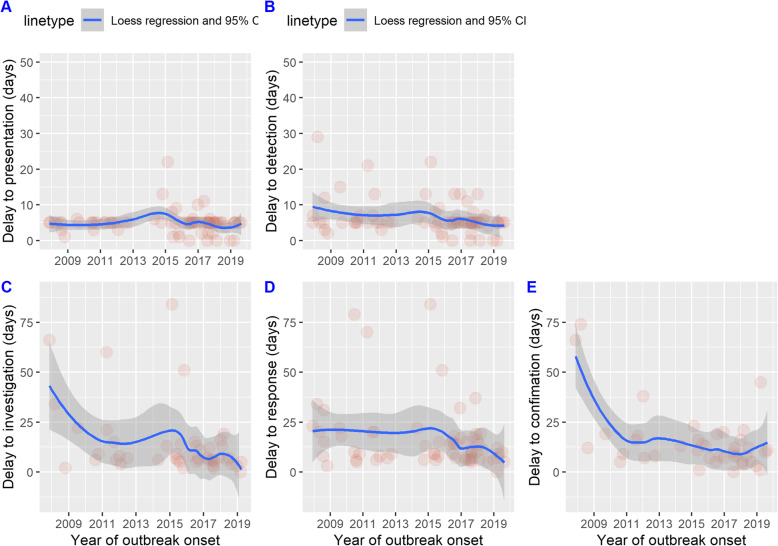
Seventy-six outbreaks from 34 countries were included. Median delays spanned 1-2 weeks: from symptom onset of the primary case to presentation at the health facility (5 days, IQR 5-5), detection (5 days, IQR 5-6), investigation (7 days, IQR 5.8-13.3), response (10 days, IQR 7-18), and confirmation (11 days, IQR 7-16). In the model simulation, the median delay to response (10 days) with 3 seed cases led to a median epidemic size of 12 cases (upper range, 47) and 8% of outbreaks ≥ 20 cases (increasing to 32% with a 30-day delay to response). Increased outbreak size at detection (10 seed cases) and a 10-day median delay to response resulted in an epidemic size of 34 cases (upper range 67 cases) and < 1% of outbreaks < 20 cases. We estimated an annual global decrease in delay to response of 5.2% (95% CI 0.5-9.6, p = 0.03). Outbreaks signaled by immediate alerts were associated with a reduction in delay to response of 39.3% (95% CI 5.7-61.0, p = 0.03).
From 2008 to 2019, median delays from symptom onset of the primary case to case presentation and to response were 5 days and 10 days, respectively. Our model simulations suggest that depending on the outbreak size (3 versus 10 seed cases), in 8 to 99% of scenarios, a 10-day delay to response would result in large clusters that would be difficult to contain. Improving the delay to response involves rethinking the integration at local levels of event-based detection, rapid diagnostic testing for cluster validation, and integrated alert, investigation, and response.
霍乱疫情不断对疾病防控提出挑战,尤其是在脆弱和受冲突影响的国家。在疫情蔓延之前,快速发现和应对小规模霍乱集群是进行有效控制的关键。为了了解脆弱国家的早期应对能力,我们调查了疫情发现、调查、应对和实验室确认方面的延迟,并估计了疫情规模。我们评估了延迟的预测因素以及应对时间的年度变化。
我们从 2008 年至 2019 年期间编制了脆弱和受冲突影响国家的霍乱疫情清单。我们搜索了同行评议的文章和流行病学报告。我们评估了从主要病例症状出现到疫情发现、调查、应对和确认的最早日期的延迟。概述了如何发出疫情警报的信息。使用分支过程模型估计每次延迟的疫情规模。使用回归模型调查预测因素与应对延迟之间的关联。
纳入了来自 34 个国家的 76 次暴发。中位延迟跨越 1-2 周:从主要病例的症状出现到就诊于医疗机构(5 天,IQR 5-5),发现(5 天,IQR 5-6),调查(7 天,IQR 5.8-13.3),应对(10 天,IQR 7-18)和确认(11 天,IQR 7-16)。在模型模拟中,应对的中位延迟(10 天)导致 3 个种子病例的中位疫情规模为 12 例(上限为 47 例),并且 8%的疫情规模≥20 例(如果应对延迟 30 天,该比例增加到 32%)。发现时的疫情规模增加(10 个种子病例)和应对的中位延迟为 10 天,导致疫情规模为 34 例(上限为 67 例),并且<1%的疫情规模<20 例。我们估计,全球应对延迟的年度降幅为 5.2%(95%CI 0.5-9.6,p=0.03)。通过即时警报发出的疫情与应对延迟减少 39.3%相关(95%CI 5.7-61.0,p=0.03)。
从 2008 年至 2019 年,从主要病例症状出现到就诊和应对的中位延迟分别为 5 天和 10 天。我们的模型模拟表明,根据疫情规模(3 个还是 10 个种子病例),在 8%至 99%的情况下,10 天的应对延迟将导致难以控制的大型集群。改善应对延迟需要重新考虑在地方一级以事件为基础的检测、用于验证集群的快速诊断测试以及综合警报、调查和应对的整合。