Wayne State University, Detroit, MI, United States.
Georgia State University, Atlanta, GA, United States.
JMIR Public Health Surveill. 2021 Jan 8;7(1):e21327. doi: 10.2196/21327.
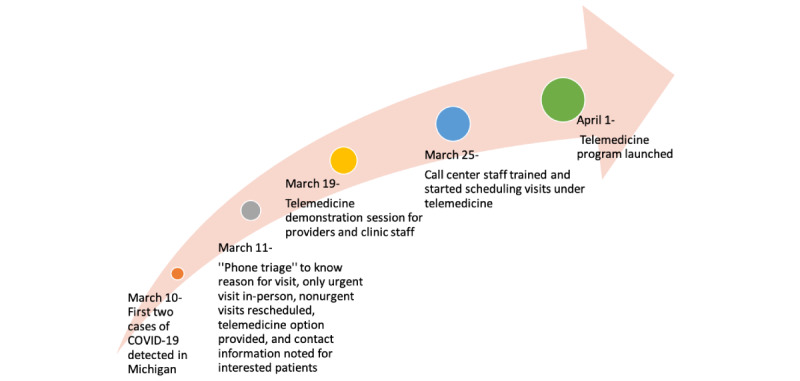
The COVID-19 pandemic, caused by SARS-CoV-2, has forced the health care delivery structure to change rapidly. The pandemic has further widened the disparities in health care and exposed vulnerable populations. Health care services caring for such populations must not only continue to operate but create innovative methods of care delivery without compromising safety. We present our experience of incorporating telemedicine in our university hospital-based outpatient clinic in one of the worst-hit areas in the world.
Our goal is to assess the adoption of a telemedicine service in the first month of its implementation in outpatient practice during the COVID-19 pandemic. We also want to assess the need for transitioning to telemedicine, the benefits and challenges in doing so, and ongoing solutions during the initial phase of the implementation of telemedicine services for our patients.
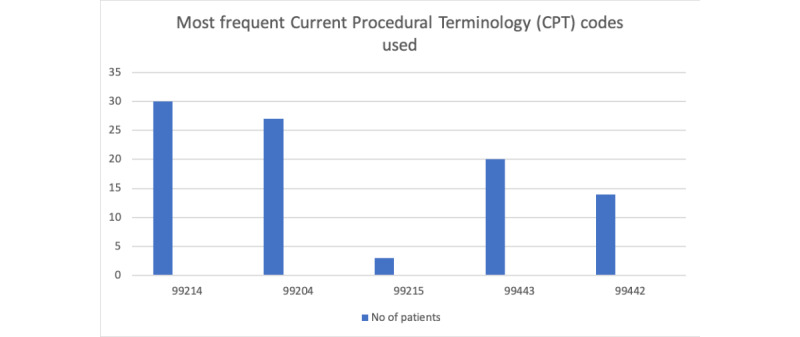
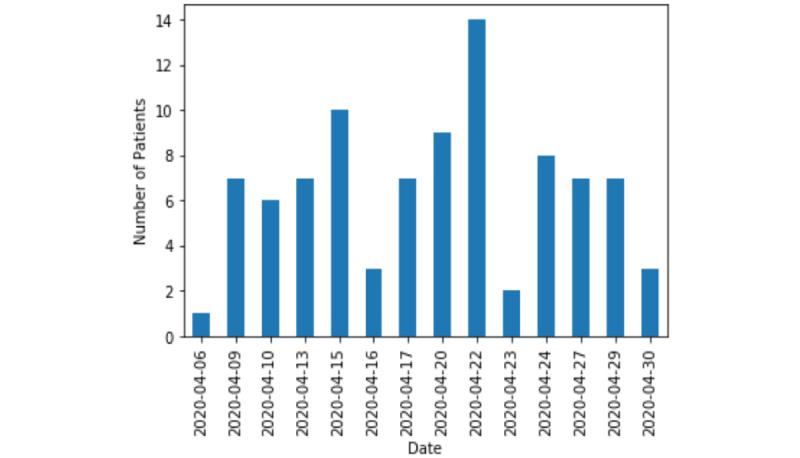
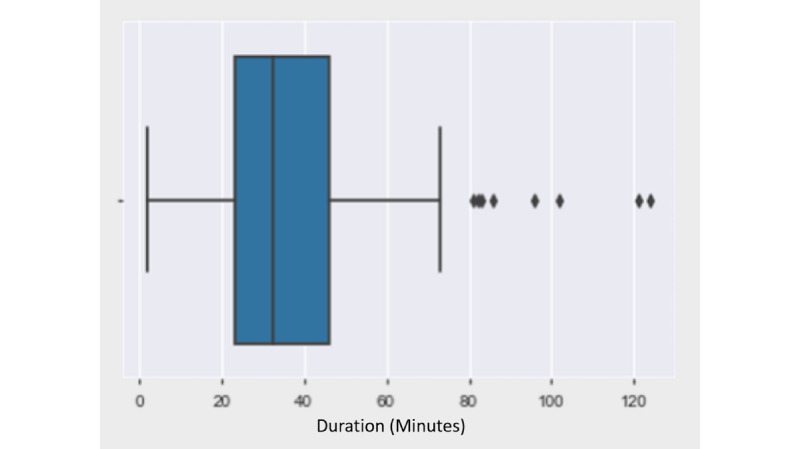
We conducted a prospective review of clinic operations data from the first month of a telemedicine rollout in the outpatient adult ambulatory clinic from April 1, 2020, to April 30, 2020. A telemedicine visit was defined as synchronous audio-video communication between the provider and patient for clinical care longer than 5 minutes or if the video visit converted to a telephone visit after 5 minutes due to technical problems. We recorded the number of telemedicine visits scheduled, visits completed, and the time for each visit. We also noted the most frequent billing codes used based on the time spent in the patient care and the number of clinical tasks (eg, activity suggested through diagnosis or procedural code) that were addressed remotely by the physicians.
During the study period, we had 110 telemedicine visits scheduled, of which 94 (85.4%) visits were completed. The average duration of the video visit was 35 minutes, with the most prolonged visit lasting 120 minutes. Of 94 patients, 24 (25.54%) patients were recently discharged from the hospital, and 70 (74.46%) patients were seen for urgent care needs. There was a 50% increase from the baseline in the number of clinical tasks that were addressed by the physicians during the pandemic.
There was a high acceptance of telemedicine services by the patients, which was evident by a high show rate during the COVID-19 pandemic in Detroit. With limited staffing, restricted outpatient work hours, a shortage of providers, and increased outpatient needs, telemedicine was successfully implemented in our practice.
由 SARS-CoV-2 引起的 COVID-19 大流行迫使医疗服务结构迅速改变。大流行进一步扩大了医疗保健方面的差距,并使弱势群体暴露无遗。照顾此类人群的医疗保健服务不仅必须继续运作,而且必须在不影响安全性的情况下创造创新的护理提供方式。我们介绍了在世界上受影响最严重的地区之一的我们的大学医院门诊中引入远程医疗的经验。
我们的目标是评估在 COVID-19 大流行期间在门诊实践中实施远程医疗服务的第一个月内采用该服务的情况。我们还希望评估过渡到远程医疗的需求,这样做的好处和挑战,以及在为我们的患者实施远程医疗服务的初始阶段的持续解决方案。
我们对 2020 年 4 月 1 日至 2020 年 4 月 30 日期间远程医疗推出后的第一个月的门诊成人门诊诊所的诊所运营数据进行了前瞻性审查。远程医疗访问被定义为提供者和患者之间进行的临床护理时间超过 5 分钟的同步音频-视频通信,或者如果由于技术问题,视频访问在 5 分钟后转换为电话访问。我们记录了预约的远程医疗访问次数、完成的访问次数以及每次访问的时间。我们还根据花费在患者护理上的时间和医生远程处理的临床任务数量(例如,通过诊断或程序代码建议的活动)记录了最常用的计费代码。
在研究期间,我们安排了 110 次远程医疗访问,其中 94 次(85.4%)访问完成。视频访问的平均持续时间为 35 分钟,最长的访问持续了 120 分钟。在 94 名患者中,有 24 名(25.54%)患者最近从医院出院,有 70 名(74.46%)患者因紧急护理需求就诊。在 COVID-19 大流行期间,医生处理的临床任务数量增加了 50%。
在底特律的 COVID-19 大流行期间,患者对远程医疗服务的接受度很高,这一点显而易见。由于人员有限、门诊工作时间受限、提供者短缺以及门诊需求增加,远程医疗在我们的实践中得到了成功实施。