Gastroenterology Hepatology and Transplantation, ASST Papa Giovanni XXIII-Bergamo, Bergamo, Italy.
Department of Infectious Diseases, IRCCS Fondazione Policlinico San Matteo, Pavia, Italy.
PLoS One. 2021 Jan 14;16(1):e0245281. doi: 10.1371/journal.pone.0245281. eCollection 2021.
Validated tools for predicting individual in-hospital mortality of COVID-19 are lacking. We aimed to develop and to validate a simple clinical prediction rule for early identification of in-hospital mortality of patients with COVID-19.
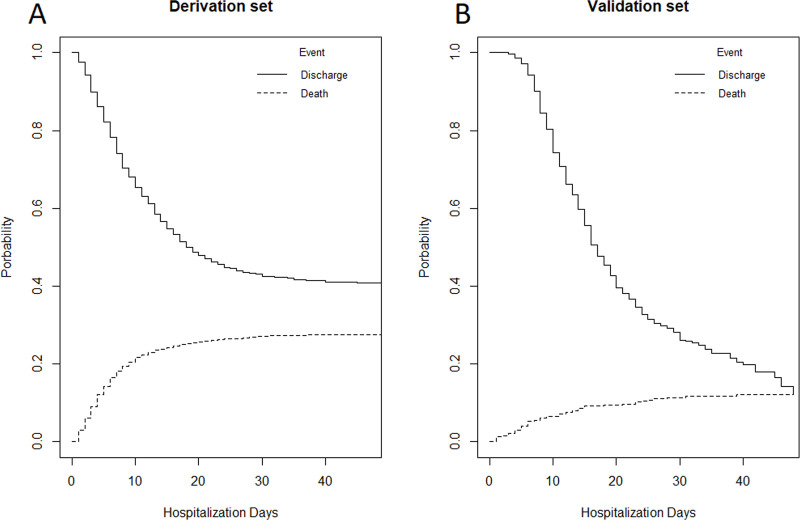
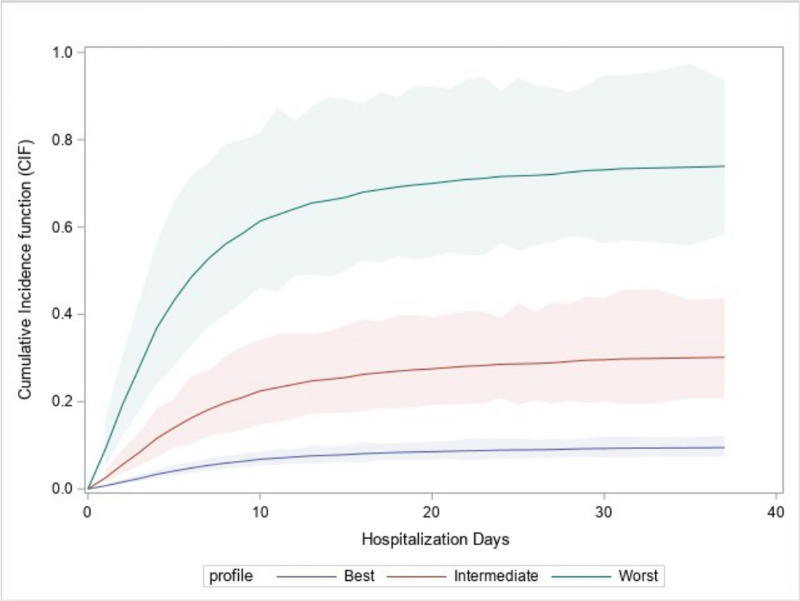
We enrolled 2191 consecutive hospitalized patients with COVID-19 from three Italian dedicated units (derivation cohort: 1810 consecutive patients from Bergamo and Pavia units; validation cohort: 381 consecutive patients from Rome unit). The outcome was in-hospital mortality. Fine and Gray competing risks multivariate model (with discharge as a competing event) was used to develop a prediction rule for in-hospital mortality. Discrimination and calibration were assessed by the area under the receiver operating characteristic curve (AUC) and by Brier score in both the derivation and validation cohorts. Seven variables were independent risk factors for in-hospital mortality: age (Hazard Ratio [HR] 1.08, 95% Confidence Interval [CI] 1.07-1.09), male sex (HR 1.62, 95%CI 1.30-2.00), duration of symptoms before hospital admission <10 days (HR 1.72, 95%CI 1.39-2.12), diabetes (HR 1.21, 95%CI 1.02-1.45), coronary heart disease (HR 1.40 95% CI 1.09-1.80), chronic liver disease (HR 1.78, 95%CI 1.16-2.72), and lactate dehydrogenase levels at admission (HR 1.0003, 95%CI 1.0002-1.0005). The AUC was 0.822 (95%CI 0.722-0.922) in the derivation cohort and 0.820 (95%CI 0.724-0.920) in the validation cohort with good calibration. The prediction rule is freely available as a web-app (COVID-CALC: https://sites.google.com/community.unipa.it/covid-19riskpredictions/c19-rp).
A validated simple clinical prediction rule can promptly and accurately assess the risk for in-hospital mortality, improving triage and the management of patients with COVID-19.
目前缺乏用于预测 COVID-19 患者院内死亡率的有效工具。本研究旨在开发并验证一种简单的临床预测规则,以早期识别 COVID-19 患者的院内死亡风险。
我们纳入了来自意大利三个专门病房的 2191 例连续住院的 COVID-19 患者(推导队列:来自贝加莫和帕维亚病房的 1810 例连续患者;验证队列:来自罗马病房的 381 例连续患者)。主要结局为院内死亡率。采用 Fine-Gray 竞争风险多变量模型(以出院为竞争事件),建立预测院内死亡率的规则。在推导队列和验证队列中,通过接受者操作特征曲线下面积(AUC)和 Brier 评分评估预测模型的区分度和校准度。7 个变量是院内死亡的独立危险因素:年龄(HR 1.08,95%CI 1.07-1.09)、男性(HR 1.62,95%CI 1.30-2.00)、入院前症状持续时间<10 天(HR 1.72,95%CI 1.39-2.12)、糖尿病(HR 1.21,95%CI 1.02-1.45)、冠心病(HR 1.40,95%CI 1.09-1.80)、慢性肝脏疾病(HR 1.78,95%CI 1.16-2.72)和入院时乳酸脱氢酶水平(HR 1.0003,95%CI 1.0002-1.0005)。推导队列的 AUC 为 0.822(95%CI 0.722-0.922),验证队列为 0.820(95%CI 0.724-0.920),校准度良好。该预测规则可作为一个免费的网络应用程序(COVID-CALC:https://sites.google.com/community.unipa.it/covid-19riskpredictions/c19-rp)使用。
验证后的简单临床预测规则可迅速、准确地评估院内死亡风险,改善 COVID-19 患者的分诊和管理。