Gagliardi Anna R, Martinez Juan Pablo Diaz, Baker G Ross, Moody Lesley, Scane Kerseri, Urquhart Robin, Wodchis Walter P
Toronto General Hospital Research Institute, University Health Network, 200 Elizabeth Street, 13EN-228, Toronto, M5G2C4, Canada.
Biostatistics Research Unit, University Health Network, Toronto, Canada.
BMC Health Serv Res. 2021 Feb 25;21(1):179. doi: 10.1186/s12913-021-06174-0.
Patient engagement (PE) in planning or improving hospital facilities or services is one approach for improving healthcare delivery and outcomes. To provide evidence on hospital capacity needed to support PE, we described the attributes of hospital PE capacity associated with clinical quality measures.
We conducted a cross-sectional survey of general and specialty hospitals based on the Measuring Organizational Readiness for Patient Engagement framework. We derived a PE capacity index measure, and with Multiple Correspondence Analysis, assessed the association of PE capacity with hospital type, and rates of hand-washing, C. difficile infection rates and 30-day readmission.
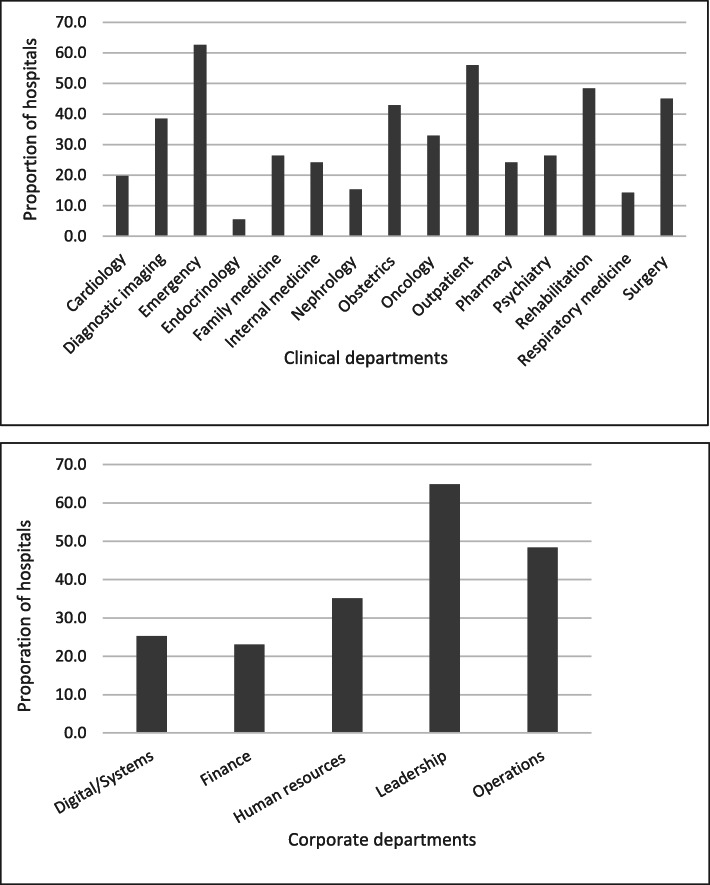
Respondents (91, 66.4%) included general: < 100 beds (48.4%), 100+ beds (27.5%), teaching hospitals (11.0%) and specialty (13.2%) hospitals. Most featured PE in multiple clinical and corporate departments. Most employed PE in a range of Planning (design/improve facilities 94.5%, develop strategic plans 87.9%), Evaluation/Quality Improvement (accreditation 91.2%, develop QI plans 90.1%) and Service Delivery activities (develop information/communication aids 92.3%). Hospitals enabled PE with multiple supports (median 12, range 0 to 25), most often: 76.9% strategic plan recognizes PE, 74.7% patient/family advisory council, and 69.2% pool of patient volunteers; and least often: 30.0% PE staff, 26.4% PE funding and 16.5% patient reimbursement or 3.3% compensation. Hospitals employed a range of less (inform, consult) and more (involve, partner) active modes of engagement. Two variables accounted for 29.6% of variance in hospital PE capacity index measure data: number of departments featuring PE and greater use of active engagement modes. PE capacity was not associated with general hospital type or clinical quality measures.
Hospitals with fewer resources can establish favourable PE conditions by deploying PE widely and actively engaging patients. Healthcare policy-makers, hospital executives and PE managers can use these findings to allocate PE resources. Future research should explore how PE modes and methods impact clinical outcomes.
让患者参与医院设施或服务的规划或改进是改善医疗服务提供和结果的一种方法。为了提供有关支持患者参与所需医院能力的证据,我们描述了与临床质量指标相关的医院患者参与能力的属性。
我们基于“衡量组织对患者参与的准备程度”框架对综合医院和专科医院进行了横断面调查。我们得出了一个患者参与能力指数测量值,并通过多重对应分析评估了患者参与能力与医院类型、洗手率、艰难梭菌感染率和30天再入院率之间的关联。
受访者(91人,占66.4%)包括综合医院:床位<100张的医院(48.4%)、床位≥100张的医院(27.5%)、教学医院(11.0%)和专科医院(13.2%)。大多数医院在多个临床和行政部门开展了患者参与活动。大多数医院在一系列规划(设计/改进设施94.5%、制定战略计划87.9%)、评估/质量改进(认证91.2%、制定质量改进计划90.1%)和服务提供活动(开发信息/沟通辅助工具92.3%)中采用了患者参与。医院通过多种支持措施来实现患者参与(中位数为12,范围为0至25),最常见的是:76.9%的战略计划认可患者参与,74.7%设有患者/家属咨询委员会,69.2%有患者志愿者库;最不常见的是:30.0%有患者参与工作人员,26.4%有患者参与资金,16.5%有患者报销或3.3%有补偿。医院采用了一系列较少(告知)和较多(参与、合作)的积极参与模式。两个变量占医院患者参与能力指数测量数据方差的29.6%:开展患者参与的部门数量以及更多地使用积极参与模式。患者参与能力与综合医院类型或临床质量指标无关。
资源较少的医院可以通过广泛开展患者参与并积极让患者参与来建立有利的患者参与条件。医疗保健政策制定者、医院管理人员和患者参与管理人员可以利用这些发现来分配患者参与资源。未来的研究应探索患者参与模式和方法如何影响临床结果。