Agho Ekhosuehi Theophilus, Owotade Foluso John, Kolawole Babatope Ayodeji, Oyetola Elijah Olufemi, Adedeji Tewogbade Adeoye
Department of Dental Surgery, Ahmadu Bello University, Zaria, 810107, Nigeria.
Department of Oral Medicine and Oral Pathology, Obafemi Awolowo University, Ile-Ife, 220005, Nigeria.
BMC Oral Health. 2021 Mar 6;21(1):101. doi: 10.1186/s12903-021-01453-y.
Type 2 diabetes mellitus has reached epidemic proportions worldwide and improved detection techniques and biomarkers are urgently needed across the spectrum of diabetes initiation and progression. Inflammatory biomarkers play a role in the development of the condition and blood is the gold standard body fluid for the diagnosis of diabetes mellitus. Serum glycated haemoglobin is a widely used marker of chronic hyperglycemia, and it is currently used to diagnose type 2 diabetes mellitus and it is the standard biomarker for the adequacy of management. However, saliva offers an alternative to serum as a biological fluid for diagnostic purposes. Non-invasive measures of inflammatory biomarkers (such as saliva diagnostics) are increasingly being investigated due to significant similarities between salivary and serum proteome. The role of saliva diagnostics in diabetes mellitus has not been explored in our study population.
This study investigated the association of selected salivary inflammatory biomarkers (Interleukin 6 [IL-6], C-reactive protein [CRP], and Tumour necrosis factor α [TNF-α]) to glycated haemoglobin (HbA1C) in type 2 diabetics.
Seventy-five participants, 39 type 2 diabetics (52%) and 36 (48%) healthy controls were recruited. Saliva and blood samples were collected for each participant. The levels of selected salivary inflammatory biomarkers (IL-6, CRP and TNF-α) were estimated by Enzyme Linked Immunosorbent Assay (ELISA) method and glycated haemogloin (HbA1C) was estimated using the liquid chromatography method. Periodontal status of the participants were determined using the Basic Periodontal Examination (BPE).
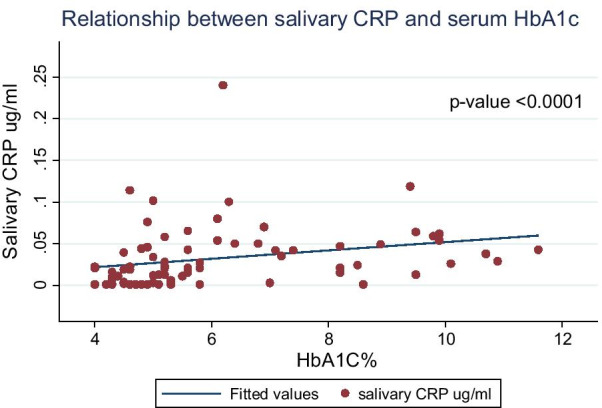
The mean salivary levels of CRP was significantly higher in diabetics, 0.05 ± 0.04 µg/ml than in controls, 0.02 ± 0.02 µg/ml (p < 0.001). Mean TNF-α was also significantly higher in diabetics, 5.39 ± 12.10 pg/ml than in controls, 1.51 ± 3.66 pg/ml (p = 0.036). Mean salivary IL-6 was also higher in diabetics compared with controls (47.20 ± 18.49 versus 41.94 ± 16.88 pg/ml), but the difference was not statistically significant, p = 0.204. In the multivariate analysis adjusting for age and periodontal status, only the mean salivary CRP was significantly higher in diabetics, 0.034 higher than controls (95% CI 0.009, 0.059 and p = 0.01). There was a positive correlation between salivary CRP and HbA1C levels, which was moderate with r-value 0.4929 and p-value < 0.0001.
Salivary inflammatory biomarkers especially CRP are higher in diabetics compared with controls and CRP is positively correlated with serum HbA1C levels. The biomarkers show potentials as non-invasive alternative method to evaluate glycaemic control in diabetes.
2型糖尿病在全球范围内已呈流行态势,在糖尿病发生和发展的各个阶段,迫切需要改进检测技术和生物标志物。炎症生物标志物在该疾病的发展过程中发挥作用,血液是诊断糖尿病的金标准体液。血清糖化血红蛋白是广泛应用的慢性高血糖标志物,目前用于诊断2型糖尿病,也是管理是否充分的标准生物标志物。然而,唾液可作为一种替代血清的生物体液用于诊断目的。由于唾液蛋白质组与血清蛋白质组存在显著相似性,炎症生物标志物的非侵入性检测方法(如唾液诊断)正越来越多地得到研究。在我们的研究人群中,尚未探讨唾液诊断在糖尿病中的作用。
本研究调查了2型糖尿病患者中选定的唾液炎症生物标志物(白细胞介素6 [IL-6]、C反应蛋白[CRP]和肿瘤坏死因子α [TNF-α])与糖化血红蛋白(HbA1C)之间的关联。
招募了75名参与者,其中39名2型糖尿病患者(52%)和36名(48%)健康对照者。为每位参与者采集唾液和血液样本。采用酶联免疫吸附测定(ELISA)法测定选定的唾液炎症生物标志物(IL-6、CRP和TNF-α)水平,采用液相色谱法测定糖化血红蛋白(HbA1C)水平。使用基本牙周检查(BPE)确定参与者的牙周状况。
糖尿病患者的唾液CRP平均水平显著高于对照组,分别为0.05±0.04μg/ml和0.02±0.02μg/ml(p<0.001)。糖尿病患者的平均TNF-α也显著高于对照组,分别为5.39±12.10pg/ml和1.51±3.66pg/ml(p=0.036)。糖尿病患者的唾液IL-6平均水平也高于对照组(47.20±18.49对41.94±16.88pg/ml),但差异无统计学意义,p=0.204。在对年龄和牙周状况进行校正的多变量分析中,仅糖尿病患者的唾液CRP平均水平显著高于对照组,比对照组高0.034(95%CI 0.009,0.059,p=0.01)。唾液CRP与HbA1C水平呈正相关,相关性中等,r值为0.4929,p值<0.0001。
与对照组相比,糖尿病患者的唾液炎症生物标志物尤其是CRP更高,且CRP与血清HbA1C水平呈正相关。这些生物标志物显示出作为评估糖尿病血糖控制的非侵入性替代方法的潜力。